William Ronald Dodds Fairbairn: Major Concepts
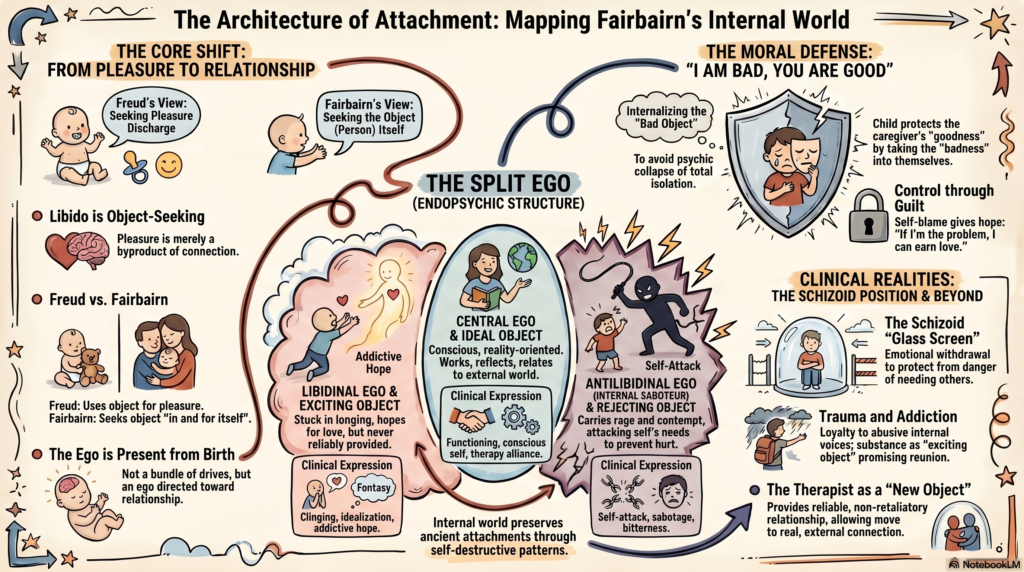 William Ronald Dodds Fairbairn, or W. R. D. Fairbairn, was one of the most important figures in British object relations theory. His central shift was this: human beings are not primarily pleasure-seeking organisms; they are object-seeking, meaning they are fundamentally driven toward relationship, attachment, and connection. His major work, Psychoanalytic Studies of the Personality, first published in 1952, helped reorient psychoanalysis toward the infant’s need for relationships and the internal world created from early relational experience.
William Ronald Dodds Fairbairn, or W. R. D. Fairbairn, was one of the most important figures in British object relations theory. His central shift was this: human beings are not primarily pleasure-seeking organisms; they are object-seeking, meaning they are fundamentally driven toward relationship, attachment, and connection. His major work, Psychoanalytic Studies of the Personality, first published in 1952, helped reorient psychoanalysis toward the infant’s need for relationships and the internal world created from early relational experience.
1. Libido is object-seeking, not pleasure-seeking
Classical Freudian theory viewed libido as primarily seeking discharge, pleasure, and tension reduction. Fairbairn disagreed.
For Fairbairn, the basic human drive is not pleasure but relationship.
A child does not love the mother because she provides pleasure. The child seeks pleasure because it is part of being connected to the loved object.
So the major correction is:
Freud:
The infant seeks pleasure and uses the object to get pleasure.
Fairbairn:
The infant seeks the object itself; pleasure follows from contact with the object.
The British Psychoanalytical Society summarizes Fairbairn’s position as the idea that libido does not merely use the object for discharge, but seeks the object “in and for itself”; pleasure is not the goal in itself, but follows from attaining the desired object.
Clinical relevance:
Many patients do not simply seek “symptom relief.” They seek an object: someone to be seen by, held in mind by, understood by, loved by, or rescued by. Even self-destructive patterns may be attempts to preserve a relationship with an internal object.
2. The ego is present from the beginning
Fairbairn rejected the idea that the infant begins as a bundle of instinctual drives and only later develops an ego. He saw the infant as having an ego from the start, already directed toward relationship.
This is important because Fairbairn’s psychology begins not with instinctual discharge but with the infant in relation to the object.
The infant’s mind is shaped by early relational experience: care, deprivation, rejection, inconsistency, seduction, over-excitement, intrusion, or emotional absence.
3. Dependence is central to development
Fairbairn gave great importance to infantile dependence.
The child is not just biologically dependent on the caregiver; the child is psychologically dependent on the caregiver’s emotional availability.
When dependence is met with care, the child develops a more integrated ego.
When dependence is met with rejection, inconsistency, neglect, or emotional unavailability, the child faces a terrible dilemma:
“I need this object, but this object hurts me.”
This dilemma becomes the foundation of internal splitting.
4. The bad object is internalized
One of Fairbairn’s most powerful ideas is that when the external object is bad, rejecting, depriving, or unreliable, the child does not simply give it up.
The child internalizes the bad object.
Why?
Because the child cannot afford to lose the caregiver psychologically. For the dependent child, a bad object is better than no object.
This is clinically profound.
A child may prefer:
“My mother is good, and I am bad”
rather than:
“My mother is bad, unreliable, or emotionally unavailable.”
The first belief preserves attachment. The second threatens psychic collapse.
This leads to Fairbairn’s concept of the moral defense.
5. The moral defense
The moral defense is Fairbairn’s idea that the child protects the goodness of the external object by taking badness into the self.
Instead of thinking:
“My caregiver is rejecting.”
The child feels:
“I am unlovable.”
Instead of:
“The object failed me.”
The child believes:
“I must have done something wrong.”
This protects the attachment bond.
The child preserves the needed object as good by making the self bad.
Clinical examples:
A neglected child may grow into an adult who says:
“I was too needy.”
A rejected partner may say:
“I must not be lovable enough.”
A patient from a harsh family may say:
“My parents did their best; I was the difficult one.”
The moral defense is painful, but it gives the person a sense of control. If the problem is “my badness,” then perhaps I can become good enough and finally earn love.
This is why patients often cling to guilt, shame, and self-blame. They are not merely symptoms; they are attachment-preserving strategies.
6. Splitting of the ego
Fairbairn’s model of splitting differs from Freud’s structural model of id, ego, and superego.
Fairbairn proposed that the ego itself splits in response to unbearable object relations.
The ego is divided into three broad structures:
- Central ego
- Libidinal ego
- Antilibidinal ego, also called the internal saboteur
Encyclopedia sources summarize Fairbairn’s model as involving a central ego available for real relationships, plus unconscious libidinal and antilibidinal ego structures.
7. Central ego
The central ego is the relatively conscious, reality-oriented part of the self.
It relates to the external world and to what Fairbairn called the ideal object.
The central ego is the part of the patient that comes to therapy, works, thinks, reflects, and tries to function.
In healthy development, the central ego has enough access to good object experience and can maintain realistic relationships.
In pathology, the central ego may become depleted because too much emotional energy is locked away in split-off internal object relations.
Clinical picture:
The patient may appear functional, polite, intelligent, and composed, but internally feel empty, unreal, detached, or emotionally frozen.
8. Libidinal ego
The libidinal ego is the part of the self that remains attached to the exciting, promising, desired object.
This part says:
“One day I will be loved.”
“One day they will understand me.”
“One day the unavailable object will become available.”
It is attached not to a fully good object, but to an exciting object.
The exciting object gives hope but does not truly satisfy.
Examples:
The emotionally unavailable parent who occasionally shows warmth.
The inconsistent romantic partner who alternates affection and withdrawal.
The admired but unreachable figure.
The addiction object that promises relief but gives only temporary gratification.
The libidinal ego is the hopeful, longing, waiting part of the personality.
Clinical relevance:
This explains why people remain attached to unavailable, rejecting, or intermittently rewarding objects.
The attachment is not irrational from the internal world’s point of view. The person is bound to hope.
9. Exciting object
The exciting object is the internalized version of the object that promises love, rescue, gratification, or recognition but does not reliably provide it.
It excites longing.
It creates anticipation.
It sustains fantasy.
But it does not truly nourish.
Clinical examples:
The parent who says, “I care,” but is emotionally absent.
The partner who gives intense attention briefly, then disappears.
The substance that promises relief but leads to dependence.
The achievement fantasy: “Once I succeed, I will finally be loved.”
The exciting object is powerful because it keeps the libidinal ego invested in hope.
10. Antilibidinal ego or internal saboteur
The antilibidinal ego is the part of the self that is attached to the rejecting object.
It carries anger, bitterness, hatred, contempt, humiliation, and resentment.
Fairbairn originally called it the internal saboteur. The antilibidinal ego is a split-off structure related to the rejecting object.
This is the part that attacks need.
It may say:
“Don’t be weak.”
“You are pathetic for wanting love.”
“No one will come.”
“You deserve rejection.”
“Depending on others is dangerous.”
Clinical relevance:
This concept beautifully explains self-sabotage.
A person may consciously want intimacy, success, or recovery. But internally, the antilibidinal ego attacks hope and dependency.
In therapy, this may appear as:
Missing sessions just when therapy becomes meaningful.
Mocking one’s own vulnerability.
Rejecting help before help can be withdrawn.
Destroying relationships before being abandoned.
Turning rage inward as self-hatred.
11. Rejecting object
The rejecting object is the internalized version of the unavailable, critical, humiliating, abandoning, neglectful, or depriving caregiver.
The antilibidinal ego is bound to this rejecting object.
This dyad is often full of grievance, accusation, and rage.
The person may carry an internal world in which one part of the self is forever complaining to an internal rejecting figure:
“You hurt me.”
“You never gave me what I needed.”
“You humiliated me.”
But the person cannot let go of the rejecting object because it is still an object. Even hatred preserves attachment.
12. Fairbairn’s three ego-object pairs
Fairbairn’s mature model can be simplified as three internal ego-object relationships:
| Ego part | Internal object | Emotional tone | Clinical expression |
|---|---|---|---|
| Central ego | Ideal object | Reality, adaptation, ordinary relatedness | Functioning, conscious self, therapeutic alliance |
| Libidinal ego | Exciting object | Hope, longing, fantasy | Clinging, idealization, addictive hope |
| Antilibidinal ego | Rejecting object | Rage, contempt, humiliation | Self-attack, sabotage, bitterness, rejection of need |
This is one of Fairbairn’s most clinically useful contributions: symptoms are not isolated phenomena; they are expressions of internal object relationships.
13. Schizoid position as basic psychopathology
Fairbairn gave special importance to schizoid phenomena.
By “schizoid,” he did not simply mean schizophrenia or schizoid personality disorder in the modern DSM sense. He meant a basic division in the personality caused by unbearable relational experience.
The schizoid person may experience:
Emotional withdrawal.
Fear of dependency.
Feeling unreal or cut off.
Preference for fantasy over relationship.
Fear that love is dangerous.
A sense of emptiness, deadness, or futility.
A chapter on Fairbairn describes the schizoid state as involving emptiness, deadness, futility, and feeling cut off “as though separated from the world and their own feelings by a glass screen.”
Clinical relevance:
Many patients who seem “avoidant,” “emotionally detached,” “intellectualized,” or “cold” may actually be protecting themselves from unbearable dependency needs.
The schizoid solution is:
“If needing people hurts, I will stop needing.”
But the need does not disappear. It goes underground.
14. Repression of bad objects
Fairbairn’s theory of repression is not mainly about repressing forbidden wishes.
It is about repressing bad internal objects.
The child cannot tolerate full awareness of the bad object because the object is needed.
So the bad object is internalized, split off, and repressed.
This creates internal persecutory relationships.
The person may later experience anxiety, depression, compulsions, self-hatred, relational repetition, or psychosomatic distress without knowing that these symptoms are linked to internal bad-object relations.
15. Attachment to bad objects
One of Fairbairn’s most clinically unsettling ideas is that people remain attached to bad objects.
Not because they enjoy suffering.
Not because they are masochistic in a simple sense.
But because the bad object is still an object.
A child cannot say:
“I will abandon my parents internally.”
So the child preserves the object inside.
Later, the adult may repeat the same structure:
Choosing unavailable partners.
Seeking approval from rejecting authorities.
Remaining loyal to abusive internal voices.
Feeling more familiar with criticism than kindness.
Distrusting stable love.
This is highly relevant to personality disorders, trauma bonding, addictive relationships, and chronic depression.
16. Psychopathology as disturbed object relations
For Fairbairn, psychopathology is not primarily conflict between instinct and society. It is disturbance in internalized relationships.
Symptoms arise from split-off ego-object systems.
Examples:
Depression:
The self identifies with badness to preserve the good object.
Addiction:
The substance becomes an exciting object that promises soothing and reunion.
Borderline states:
The person oscillates between longing for the exciting object and rage toward the rejecting object.
Schizoid states:
The person withdraws from external relationships into inner object relations.
Obsessive states:
Control may defend against dependency, rage, and fear of object loss.
Narcissistic vulnerability:
The self may be organized around the search for an ideal object that confirms worth.
17. Transference as real relationship plus old internal object relation
Fairbairn’s view of transference is clinically modern.
Transference is not merely a distortion projected onto a neutral analyst. It is the patient bringing internal object relations into the therapeutic relationship.
The therapist may become:
The exciting object: “You will finally rescue me.”
The rejecting object: “You don’t really care.”
The ideal object: “You are the only safe person.”
The therapist’s task is not just interpretation. The therapist also becomes a new relational experience.
Fairbairn helped move psychoanalysis away from the analyst as a detached screen and toward the idea that the therapeutic relationship itself can be transformative. Routledge’s description notes that his work remains relevant to psychoanalytic practice, infant research, group relations, and family therapy.
18. The therapist as a new object
In Fairbairn’s model, treatment involves helping the patient move from closed internal object systems toward real relationship.
The therapist provides:
Reliability.
Emotional presence.
Non-retaliation.
Recognition of dependency needs.
Interpretation of internal object relations.
A relationship that is neither exciting in a false way nor rejecting in a familiar way.
The patient gradually discovers:
“I can need without being humiliated.”
“I can be angry without destroying the relationship.”
“I can receive care without becoming weak.”
“I can relate to a real person, not only to my internal objects.”
19. Difference from Freud
| Freud | Fairbairn |
|---|---|
| Drive theory | Object relations theory |
| Libido seeks pleasure/discharge | Libido seeks the object |
| Id is central source of instinctual pressure | Ego is present from beginning |
| Conflict between instinct and prohibition | Conflict within internal object relations |
| Repression of unacceptable wishes | Repression of bad objects |
| Symptoms express drive conflict | Symptoms express split ego-object systems |
| Analyst as projection screen | Therapist as real new object |
20. Difference from Melanie Klein
Fairbairn and Klein both focused on internal objects, but they differed.
Klein:
Emphasized innate aggression, phantasy, envy, persecutory anxiety, depressive position, and the infant’s attacks on the object.
Fairbairn:
Placed more emphasis on environmental failure, dependence, rejection, and the child’s need to preserve attachment.
In simple terms:
Klein asks:
“What does the infant do to the object in phantasy?”
Fairbairn asks:
“What happens to the infant’s ego when the needed object fails?”
21. Difference from Winnicott
Winnicott focused on holding, the facilitating environment, true self and false self, transitional phenomena, and the mother’s adaptive function.
Fairbairn focused more on internal splitting caused by the need to preserve relationships with bad objects.
Winnicott:
Failure of holding leads to false self and impingement.
Fairbairn:
Failure of relationship leads to internalized bad objects and split ego structures.
Both are clinically complementary.
22. Fairbairn and trauma
Fairbairn is extremely useful in trauma work.
Many trauma survivors continue to feel attached to abusive or neglectful figures. Fairbairn helps us understand this without blaming the patient.
The survivor may internalize:
The rejecting object.
The humiliating object.
The exciting but unreliable object.
The self-blaming moral defense.
The internal saboteur.
Thus, even after external escape, the internal relationship continues.
This is why trauma therapy often requires not just remembering events, but transforming internal object relations.
23. Fairbairn and addiction
Fairbairn’s model is very useful in addiction formulation.
The addictive substance or behavior can function as an exciting object.
It promises:
Relief.
Warmth.
Confidence.
Self-soothing.
Escape from emptiness.
Reunion with a lost good object.
But over time, it becomes rejecting too.
The person then develops an internal cycle:
Longing → use → relief → shame → self-attack → renewed longing.
In Fairbairnian terms:
The libidinal ego seeks the exciting object.
The antilibidinal ego attacks the self after disappointment.
The central ego becomes weakened.
Recovery involves building real relationships and strengthening the central ego so that the person no longer has to depend on the addictive object for emotional regulation.
24. Fairbairn and borderline personality organization
Fairbairn’s ideas help explain borderline dynamics:
Intense longing for the exciting object.
Rage toward the rejecting object.
Fear of abandonment.
Self-sabotage through the internal saboteur.
Rapid shifts between idealization and rejection.
Difficulty holding an integrated view of self and other.
From this perspective, borderline symptoms are not merely impulsivity or emotional dysregulation. They are the expression of split internal object relations.
25. Fairbairn and depression
In depression, the moral defense is especially important.
The depressed patient may unconsciously preserve the goodness of the object by making the self bad.
Common depressive themes:
“I am a burden.”
“I ruin everything.”
“I am unlovable.”
“I don’t deserve care.”
Fairbairn would ask:
Which internal object is being protected by this self-blame?
What relationship is being preserved by guilt?
Whose badness has the patient taken into the self?
26. Fairbairn and schizoid personality
Fairbairn’s schizoid patient is not simply indifferent to relationships.
The schizoid person may intensely need relationship but fear the consequences of need.
Core conflict:
“I need the object, but needing the object exposes me to rejection, engulfment, humiliation, or disappointment.”
So the patient retreats.
They may live in:
Ideas.
Fantasy.
Work.
Intellectualization.
Private inner worlds.
Controlled, low-demand relationships.
The tragedy is that withdrawal protects the person from pain but also deepens emptiness.
27. Fairbairn’s clinical question
A Fairbairnian formulation often asks:
What object is the patient seeking?
What object is the patient afraid of?
What bad object has been internalized?
How does the patient preserve attachment through self-blame?
Which part of the ego is speaking now: central, libidinal, or antilibidinal?
Is the therapist being experienced as ideal, exciting, or rejecting?
What internal relationship is being repeated in the room?
28. Simple clinical formulation template
A Fairbairnian formulation may look like this:
The patient’s central ego is trying to function adaptively, but much of the personality remains organized around split internal object relations. The libidinal ego remains attached to an exciting but unreliable object, sustaining hope for rescue and recognition. The antilibidinal ego is identified with a rejecting internal object and attacks dependency, vulnerability, and need. The patient uses moral defense by locating badness in the self rather than recognizing the failure of early objects. Symptoms represent attempts to maintain attachment while managing rage, shame, longing, and fear of abandonment.
29. One-line summary of Fairbairn
Fairbairn teaches us that the human being is not primarily seeking pleasure, but relationship — and when real relationships fail, the mind preserves them internally, even at the cost of splitting, self-blame, sabotage, and suffering.
Key terms to remember
Object-seeking libido — human motivation is fundamentally relational.
Internal object — an internalized version of an important relationship figure.
Bad object — an internalized rejecting, depriving, or persecutory object.
Moral defense — preserving the goodness of the object by making the self bad.
Central ego — conscious, reality-oriented part of the self.
Libidinal ego — hopeful, longing part attached to the exciting object.
Antilibidinal ego/internal saboteur — angry, rejecting, self-attacking part attached to the rejecting object.
Exciting object — object that promises love but does not reliably satisfy.
Rejecting object — object experienced as humiliating, abandoning, depriving, or critical.
Schizoid position — withdrawal from external relationships because need itself has become dangerous.
Endopsychic structure — the internal organization of ego-object relationships.
Most clinically useful takeaway
Fairbairn helps us understand why patients cling to what hurts them.
They are not simply irrational.
They are preserving attachment.
A painful object may still feel safer than no object. A rejecting inner voice may still feel like a relationship. Self-blame may feel more tolerable than recognizing that the needed object failed.
That is the depth and clinical beauty of Fairbairn.