Pramipexole for Depression in Parkinson’s Disease: Dose, Benefits, Side Effects, and Patient Selection
 Depression in Parkinson’s disease is not merely an emotional reaction to a chronic neurological illness. In many patients, it is part of the biology of Parkinson’s disease itself. Parkinson’s affects dopamine circuits involved not only in tremor, stiffness, and slowness, but also in motivation, reward, pleasure, emotional drive, sleep, and goal-directed behaviour.
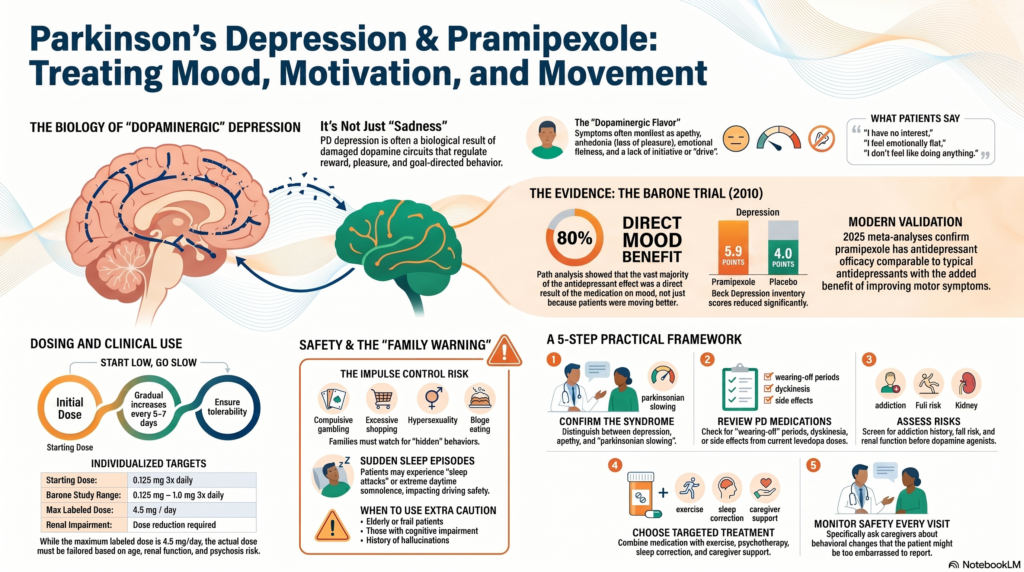
Depression in Parkinson’s disease is not merely an emotional reaction to a chronic neurological illness. In many patients, it is part of the biology of Parkinson’s disease itself. Parkinson’s affects dopamine circuits involved not only in tremor, stiffness, and slowness, but also in motivation, reward, pleasure, emotional drive, sleep, and goal-directed behaviour.
This is why depression in Parkinson’s disease may not always look like “ordinary sadness.” Patients may instead say:
“I have no interest.”
“I don’t feel like doing anything.”
“I feel emotionally flat.”
“I don’t enjoy anything.”
“I am slow, tired, and withdrawn.”
“I have lost confidence.”
These symptoms can easily be mistaken for ageing, laziness, dementia, or “just Parkinson’s.” But in many patients, they represent a treatable neuropsychiatric syndrome.
Why Dopamine Matters in Parkinson’s Depression
Dopamine is usually discussed in relation to movement. But dopamine is also deeply involved in motivation, reward anticipation, pleasure, and emotional energy. When dopamine pathways are affected in Parkinson’s disease, the patient may develop low mood, apathy, anhedonia, fatigue, reduced initiative, social withdrawal, anxiety, and loss of confidence.
This creates an important clinical question: should every depressed Parkinson’s patient simply receive a conventional antidepressant, or should the Parkinson’s medication strategy also be reviewed?
The answer is individualized. Some patients need antidepressants. Some need optimization of Parkinson’s medication. Some need psychotherapy, sleep correction, exercise, caregiver support, and structured activity. Many need a combination.
The Landmark Study: Barone et al., 2010
A landmark randomized, double-blind, placebo-controlled trial by Barone and colleagues studied pramipexole in patients with mild-to-moderate Parkinson’s disease and clinically significant depressive symptoms. Patients received pramipexole or placebo for 12 weeks, and the main outcome was change in Beck Depression Inventory score.
The study found that depression scores improved more with pramipexole than placebo. Beck Depression Inventory scores reduced by about 5.9 points with pramipexole and 4.0 points with placebo. The difference was statistically significant, though modest in size. Importantly, the study also found that about 80% of the antidepressant effect appeared to be a direct effect on depressive symptoms, while only about 20% was mediated through motor improvement.
In simple terms, mood did not improve merely because the patient moved better. Pramipexole appeared to have a direct mood-related benefit in selected Parkinson’s disease patients.
What Do Newer References Suggest?
The Barone trial remains the core placebo-controlled reference, but later evidence continues to support the idea that pramipexole may help selected patients with Parkinson’s disease depression. The 2019 Movement Disorder Society evidence-based review identified treatments considered clinically useful or possibly useful for non-motor symptoms such as depression, apathy, impulse-control disorders, dementia, psychosis, and sleep-related problems in Parkinson’s disease.
A 2022 meta-analysis reported that pramipexole may improve treatment efficacy and Hamilton Depression Rating Scale scores in Parkinson’s disease patients with anxiety or depression. A newer meta-analysis comparing pramipexole with antidepressants concluded that pramipexole had antidepressant effects similar to typical antidepressants while also improving motor symptoms in Parkinson’s disease patients.
The practical conclusion is not that pramipexole should replace antidepressants. Rather, it should be considered as one possible option in carefully selected Parkinson’s disease patients, especially when depression overlaps with apathy, anhedonia, loss of motivation, psychomotor slowing, and dopaminergic features.
Dose Range of Pramipexole
Pramipexole should always be started low and increased slowly. It is not a medication to be started casually or escalated rapidly.
In the Barone trial on depression in Parkinson’s disease, pramipexole was started at 0.125 mg three times daily and titrated up to 1 mg three times daily. The mean daily dose at the final visit was around 2.18 mg/day.
For Parkinson’s disease, the usual immediate-release dosing schedule begins at 0.125 mg three times daily, with gradual increases every 5–7 days if required and tolerated. The labelled maximum dose is 1.5 mg three times daily, or 4.5 mg/day. Pramipexole requires dose adjustment in renal impairment, and if used along with levodopa, the levodopa dose may sometimes need reduction if dyskinesia or hallucinations emerge.
| Situation | Practical dose concept |
|---|---|
| Usual starting dose in Parkinson’s disease | 0.125 mg three times daily |
| Barone depression-in-PD study range | 0.125–1 mg three times daily |
| Common effective Parkinson’s range | 1.5–4.5 mg/day in divided doses |
| Maximum labelled Parkinson’s dose | 4.5 mg/day |
| Renal impairment | Dose reduction required |
| With levodopa | Watch for dyskinesia, hallucinations, sleepiness |
These doses are for clinical understanding and patient education. The actual dose must be decided by the treating neurologist or psychiatrist based on age, renal function, cognition, psychosis risk, motor status, sleepiness, and caregiver observations.
Side Effects of Pramipexole
Pramipexole can be useful, but it is not a casual antidepressant. It is a dopamine agonist and can cause neurological, psychiatric, behavioural, sleep-related, and autonomic side effects.
Common side effects include:
- nausea
- dizziness
- sleepiness
- fatigue
- constipation
- insomnia
- abnormal dreams
- dry mouth
- confusion
- postural hypotension
- dyskinesia, especially with levodopa
- hallucinations, especially in older or cognitively vulnerable patients
The prescribing information highlights sudden sleep episodes, orthostatic hypotension, impulse-control or compulsive behaviours, hallucinations or psychotic-like behaviour, and dyskinesia as important warnings. Common adverse reactions in early Parkinson’s disease include nausea, dizziness, somnolence, insomnia, constipation, weakness, and hallucinations; in advanced Parkinson’s disease with levodopa, dyskinesia, orthostatic hypotension, hallucinations, confusion, gait problems, dry mouth, amnesia, and urinary frequency are also described.
In the Barone trial, common adverse events with pramipexole included nausea, headache, dizziness, somnolence, dyskinesia, vertigo, fatigue, and insomnia. Treatment-related hallucination occurred in 4% of the pramipexole group compared with 1% of the placebo group.
The Most Important Family Warning: Impulse-Control Disorders
The side effect that families must be specifically warned about is impulse-control disorder. Dopamine agonists can trigger or worsen behaviours such as:
- compulsive gambling
- excessive shopping
- hypersexuality
- binge eating
- compulsive internet or mobile use
- repetitive reward-seeking behaviour
NICE advises that impulse-control disorders can occur with dopaminergic therapy at any stage of Parkinson’s disease, with increased risk during dopamine agonist therapy. NICE also recommends that patients and families should be given oral and written information about this risk, including the fact that these behaviours may be concealed by the affected person.
This is clinically crucial. The patient may not report these symptoms because of embarrassment, secrecy, lack of insight, or because the behaviour itself feels rewarding. A good clinical review should ask both the patient and the caregiver.
Who Needs Extra Caution?
Pramipexole should be used with caution, or sometimes avoided, in patients with:
- hallucinations or delusions
- dementia or significant cognitive impairment
- previous gambling, addiction, or impulsive behaviour
- severe daytime sleepiness or sleep attacks
- recurrent falls or postural hypotension
- advanced frailty
- renal impairment
- active psychosis or mania
- poor family supervision
- high-risk driving or machinery use
Older adults with Parkinson’s disease often have multiple vulnerabilities: cognitive changes, sleep problems, blood pressure fluctuations, falls, constipation, polypharmacy, and caregiver burden. In such patients, every medication decision must balance benefit and harm.
Depression, Apathy, or Parkinsonian Slowing?
One of the hardest clinical tasks is separating depression from apathy and parkinsonian slowing.
Depression usually involves sadness, hopelessness, guilt, anxiety, negative thoughts, sleep disturbance, and sometimes suicidal ideas.
Apathy involves reduced initiative, reduced emotional engagement, and reduced goal-directed behaviour.
Parkinsonian slowing involves bradykinesia, reduced facial expression, soft speech, delayed responses, and fatigue.
Anhedonia involves reduced pleasure and reward sensitivity.
In real-world Parkinson’s care, these often overlap. A patient may look depressed but actually have apathy. Another may look apathetic but have severe depression. Another may have depression worsened by poor sleep, pain, constipation, wearing-off, or caregiver stress.
This is why treatment should not be based on a five-minute impression. It requires a structured neuropsychiatric assessment.
A Practical Treatment Framework
A good treatment plan for depression in Parkinson’s disease should include:
- Confirm the syndrome
Is it depression, apathy, anxiety, cognitive decline, sleep disorder, psychosis, medication side effect, or a mixture? - Review Parkinson’s medication
Look for wearing-off, dyskinesia, hallucinations, daytime sleepiness, autonomic symptoms, and timing of levodopa. - Assess risk before dopamine agonists
Screen for impulse-control behaviours, addictions, hallucinations, cognitive impairment, falls, renal impairment, and caregiver supervision. - Choose treatment individually
Options may include antidepressants, pramipexole or other Parkinson’s medication optimization, psychotherapy, behavioural activation, exercise, sleep correction, pain treatment, and caregiver psychoeducation. - Monitor outcome
Use rating scales, patient reports, caregiver feedback, and functional markers such as activity level, sleep, appetite, social engagement, and daily routine. - Monitor safety at every visit
Specifically ask about gambling, shopping, sexual behaviour, binge eating, internet use, hallucinations, dizziness, falls, and daytime sleepiness.
Take-Home Message
Depression in Parkinson’s disease is common, disabling, and often under-recognized. It is not merely sadness. It may reflect changes in dopamine-based brain circuits that regulate motivation, pleasure, emotional energy, and reward.
Pramipexole has evidence for improving depressive symptoms in selected Parkinson’s disease patients. The landmark Barone trial suggested a direct antidepressant effect, and newer meta-analytic evidence supports its possible role in Parkinson’s disease depression. However, the benefit must be weighed against important risks such as sleepiness, hallucinations, orthostatic hypotension, dyskinesia, and impulse-control disorders.
The right question is not: “Is pramipexole good or bad?”
The right question is: “Is this the right patient, at the right stage, with the right symptom profile, under the right supervision?”
Parkinson’s care should not stop with tremor and stiffness. Mood, motivation, sleep, memory, behaviour, and caregiver burden are equally important. Treating Parkinson’s well means treating the whole person.
Consultation
For comprehensive assessment and management of depression, anxiety, sleep problems, memory issues, behavioural changes, and medication-related psychiatric concerns in Parkinson’s disease:
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery
Opp. Phoenix Mall, Chennai
✉ srinivasaiims@gmail.com
📞 +91-8595155808