Early ADHD Diagnosis Can Change a Child’s Educational Trajectory
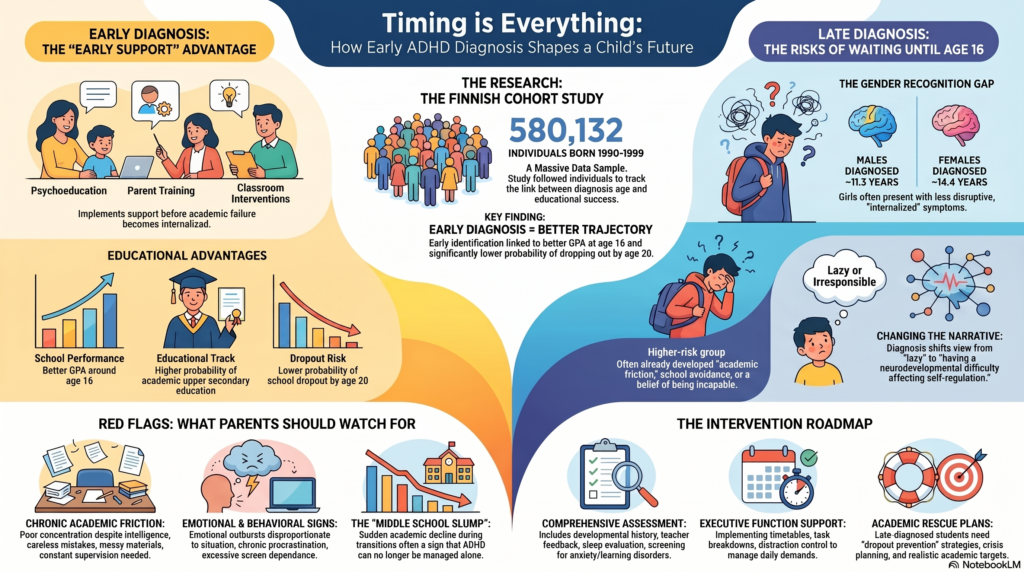 A large JAMA Psychiatry 2026 cohort study by Volotinen and colleagues followed 580,132 individuals born in Finland between 1990 and 1999 and examined whether the age at first ADHD diagnosis was associated with later educational outcomes. The key finding was clinically important: children diagnosed earlier with ADHD had better school performance, were more likely to enter academic rather than vocational tracks, and had lower school dropout rates by age 20 compared with those diagnosed near the end of compulsory schooling.
A large JAMA Psychiatry 2026 cohort study by Volotinen and colleagues followed 580,132 individuals born in Finland between 1990 and 1999 and examined whether the age at first ADHD diagnosis was associated with later educational outcomes. The key finding was clinically important: children diagnosed earlier with ADHD had better school performance, were more likely to enter academic rather than vocational tracks, and had lower school dropout rates by age 20 compared with those diagnosed near the end of compulsory schooling.
Why this study matters
ADHD is not merely a “concentration problem.” It affects attention regulation, impulse control, emotional regulation, planning, time management, working memory, and academic consistency. A bright child with untreated ADHD may still struggle with incomplete work, careless mistakes, poor exam preparation, emotional outbursts, low self-esteem, and repeated negative feedback from adults.
The Finnish study shows that timing matters. Earlier diagnosis may allow the child, family, and school to understand the pattern early and put supports in place before academic failure becomes repeated, internalised, and demoralising.
Main findings of the study
The study found that ADHD diagnosis at any age was associated with poorer educational outcomes compared with no ADHD diagnosis. However, within the ADHD group, earlier diagnosis was associated with relatively better outcomes.
Children diagnosed earlier had:
| Outcome | Earlier ADHD diagnosis was associated with |
|---|---|
| School performance | Better GPA around age 16 |
| Educational track | Higher probability of academic upper secondary education |
| Dropout | Lower probability of school dropout by age 20 |
| Late diagnosis | Higher risk group, especially when first diagnosed near age 16 |
The sex difference was also notable. In the cohort, males were diagnosed more often and earlier; mean age at first diagnosis was 11.3 years in males and 14.4 years in females. This fits a common clinical concern: girls, especially those with predominantly inattentive ADHD, are often recognised later because they may be less disruptive and more internally distressed.
The practical message: diagnosis is not labelling; it is access to support
Many parents fear that an ADHD diagnosis will “label” the child. But an accurate diagnosis, when done carefully, can reduce shame. It changes the narrative from:
“This child is lazy, careless, careless, irresponsible.”
to:
“This child has a neurodevelopmental difficulty that affects self-regulation, and we can build systems to help.”
Early diagnosis opens the door to:
- Psychoeducation for the child and family
- Parent training and behavioural strategies
- Teacher-led classroom interventions and school supports
- Medication when clinically indicated
- Screening for learning disorders, anxiety, depression, sleep problems, and substance use
- Academic planning before board exams and major transitions
Current guidelines and public health recommendations emphasise that ADHD care should not be limited to medication alone; school support, behavioural strategies, and family involvement are important parts of treatment.
The danger of late diagnosis
A child diagnosed only around age 15 or 16 has often already accumulated years of academic friction. By then, the child may have developed:
- repeated failure experiences
- low self-esteem
- oppositional reactions
- anxiety about studies
- depression or demoralisation
- excessive gaming or digital escape
- school avoidance
- substance use in some adolescents
- a belief that “I am not capable”
This is why late diagnosis should not be treated casually. It is not enough to simply prescribe medication and ask the student to study harder. A late-diagnosed adolescent needs a dropout-prevention and academic rescue plan.
A more nuanced interpretation: early diagnosis may not be the only explanation
The JAMA Psychiatry article also received an important comment on heterogeneous ADHD trajectories. Narita and colleagues argued that age at diagnosis may reflect not only access to care, but also different underlying ADHD developmental pathways. Some children have classic childhood-onset ADHD. Others are diagnosed later because symptoms become more impairing during adolescence, or because they have different comorbidity patterns.
This is important because late-diagnosed ADHD may represent a clinically distinct subgroup in some cases. A large Nature Genetics study found that late-diagnosed ADHD had a larger genetic overlap with depression than childhood ADHD, suggesting that age at diagnosis may partly reflect underlying heterogeneity rather than merely delay in recognition.
So the correct clinical interpretation is balanced:
Earlier diagnosis may improve outcomes by enabling earlier support.
But age at diagnosis may also reflect differences in severity, comorbidity, family context, school environment, and developmental trajectory.
What clinicians should do
For children and adolescents with suspected ADHD, assessment should be comprehensive. It should include:
- developmental history
- school history and teacher feedback
- parent and child interviews
- rating scales
- assessment of sleep, anxiety, depression, substance use, screen addiction, and family stress
- evaluation for learning disorders
- functional impairment across home, school, and social settings
- review of academic trajectory, not just current symptoms
For adolescents diagnosed late, the treatment plan should include a specific educational strategy:
| Area | Intervention |
|---|---|
| Attention | Medication if indicated, study blocks, distraction control |
| Executive function | Timetables, reminders, task breakdown |
| Emotional regulation | CBT/DBT-informed coping skills |
| School support | Teacher coordination, realistic academic targets |
| Dropout prevention | Frequent review, crisis planning, parental involvement |
| Comorbidity | Treat anxiety, depression, sleep problems, substance use |
What parents should watch for
Parents should consider an ADHD evaluation when a child repeatedly shows:
- poor concentration despite good intelligence
- chronic procrastination
- careless mistakes
- messy notebooks or lost materials
- emotional outbursts disproportionate to the situation
- inability to complete homework without supervision
- exam underperformance despite preparation
- excessive screen dependence
- constant negative feedback from teachers
- sudden academic decline during middle school or high school
The goal is not to pathologise normal childhood behaviour. The goal is to identify when symptoms are persistent, impairing, and present across settings.
Indian context
In India, many children are brought for assessment only after academic decline becomes severe, often around board exams, NEET/JEE preparation, or college transition. By then, the child may already carry years of criticism. The lesson from this study is clear: waiting until the child fails repeatedly is not a neutral decision.
Early ADHD assessment can protect not only marks, but also confidence, family relationships, emotional health, and long-term educational continuity.
Conclusion
The Volotinen et al. study strengthens an important clinical message: early ADHD diagnosis can be educationally protective when it leads to timely support. But it also reminds us that late-diagnosed ADHD should be taken seriously, because it may represent a subgroup with greater academic, emotional, and developmental complexity.
The best approach is neither overdiagnosis nor denial. It is careful assessment, early recognition, school collaboration, and personalised intervention.
For comprehensive ADHD assessment and treatment in Chennai
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery
Opp. Phoenix Mall, Chennai
✉ srinivasaiims@gmail.com 📞 +91-8595155808