Opioid Dose Equivalents in Clinical Practice: Bridging Heroin Use to Buprenorphine-Based OST
 In addiction psychiatry, one of the most frequent and complex clinical questions is:
In addiction psychiatry, one of the most frequent and complex clinical questions is:
👉 “How much buprenorphine is equivalent to the opioid the patient is using?”
This question arises most often in individuals using Heroin, but also in those dependent on prescription opioids like Tramadol.
While the idea of “dose equivalence” is appealing, the reality is more nuanced. In Opioid Substitution Therapy (OST), we are not merely replacing one opioid with another—we are stabilizing receptor systems, reducing harm, and restoring function.
This article provides a practical framework to understand opioid equivalence and safely transition to Buprenorphine.
🔹 Why Dose Equivalence Is Not Straightforward
In general medicine, dose equivalence implies:
- Predictable pharmacology
- Linear conversion
In opioid addiction, this breaks down due to:
1. Variable Purity (Especially Heroin)
- Street heroin may range from 10% to 60% purity
- Adulterants (caffeine, talc, fentanyl analogues) alter effects
👉 A “1 gram/day heroin user” is not a standardized unit
2. Tolerance and Receptor Adaptation
- Chronic use → receptor downregulation
- Same dose produces vastly different effects across patients
3. Pharmacological Differences
- Full agonists (heroin, morphine)
- Partial agonist (buprenorphine)
👉 This makes direct equivalence non-linear
🔹 Understanding Heroin Exposure (Clinical Approximation)
Although exact equivalence is impossible, rough clinical estimates help guide induction.
Typical Patterns (Indian Context)
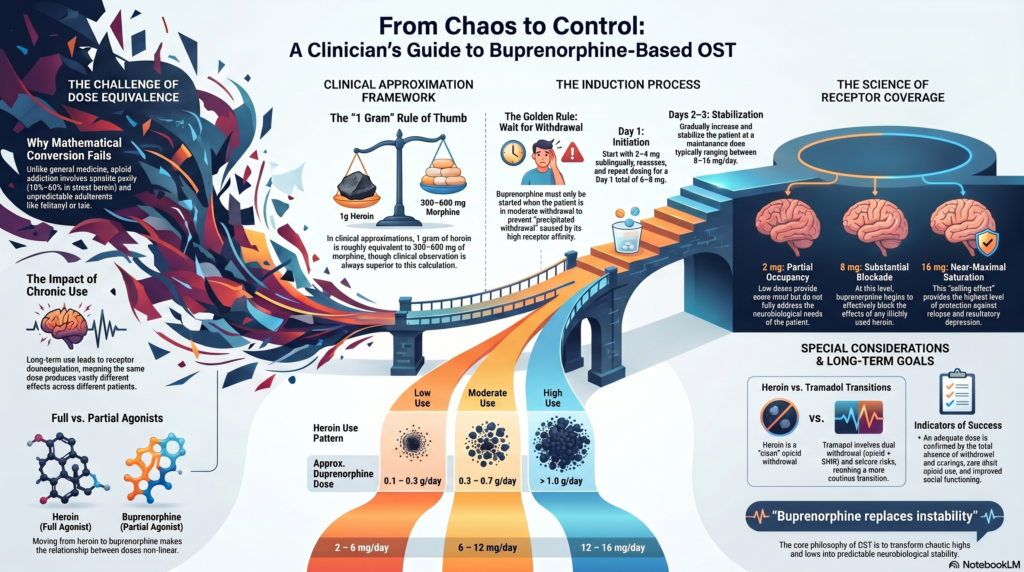
- Low use: 0.1–0.3 g/day
- Moderate: 0.3–0.7 g/day
- High: 1 g/day or more
Approximate morphine equivalent:
- 1 g heroin ≈ 300–600 mg morphine equivalent (very rough)
👉 This wide range highlights why clinical observation > mathematical conversion
🔹 Buprenorphine: A Different Kind of Opioid
Buprenorphine behaves differently from heroin.
Key Pharmacological Properties
- Partial μ-agonist
- Very high receptor affinity
- Ceiling effect on respiratory depression
This means:
- It displaces heroin
- But produces a controlled, stabilizing effect
🔹 Practical Dose Equivalence: What Actually Works
Instead of strict equivalence, clinicians use functional matching:
👉 “What dose of buprenorphine prevents withdrawal and craving?”
🔸 Rough Clinical Guide
| Heroin Use Pattern | Approximate Buprenorphine Dose |
|---|---|
| Low (0.1–0.3 g/day) | 2–6 mg/day |
| Moderate (0.3–0.7 g/day) | 6–12 mg/day |
| High (>1 g/day) | 12–16 mg/day |
⚠️ Important:
- These are starting frameworks, not prescriptions
- Always titrate based on:
- Withdrawal
- Craving
- Sedation
🔹 Induction: The Critical Step
The Rule
Start buprenorphine only when:
- Patient is in moderate withdrawal
Why?
- Prevents precipitated withdrawal
Typical Induction Pattern
Day 1
- Start: 2–4 mg SL
- Reassess → repeat dosing
Day 1 total
- Usually 6–8 mg
Day 2–3
- Stabilize:
- 8–16 mg/day
🔹 The Concept of “Receptor Coverage”
A more useful concept than equivalence is:
👉 Receptor occupancy
- ~2 mg buprenorphine → partial occupancy
- ~8 mg → substantial blockade
- ~16 mg → near-maximal receptor saturation
Clinical implication:
- Higher doses block heroin effects
- Reduce relapse risk
🔹 Harm Reduction: The Core Philosophy of OST
Programs led by National AIDS Control Organisation and National Drug Dependence Treatment Centre emphasize:
Goals of OST
- Reduce illicit opioid use
- Prevent overdose
- Reduce HIV/Hepatitis transmission
- Improve social functioning
👉 The aim is not immediate abstinence—it is controlled stabilization
🔹 Tramadol vs Heroin: Why the Transition Differs
While heroin is a pure opioid, tramadol adds complexity.
With Heroin
- Clean opioid withdrawal → buprenorphine works predictably
With Tramadol
- Dual withdrawal (opioid + SNRI)
- Seizure risk
- Slower, more cautious transition required
🔹 Common Clinical Mistakes
- Over-reliance on “conversion tables”
- Starting buprenorphine too early
- Underdosing → persistent cravings
- Rapid taper instead of maintenance
🔹 Maintenance: Where Real Recovery Happens
Typical Range
- 8–16 mg/day
Duration
- Months to years (individualized)
Indicators of adequate dose
- No withdrawal
- No craving
- No illicit opioid use
- Functional improvement
🔹 A Clinical Reframe
Perhaps the most important takeaway:
👉 Buprenorphine is not replacing heroin—it is replacing instability.
It transforms:
- Chaotic highs and lows
- Into predictable neurobiological stability
🔻 Final Takeaway
- Opioid “equivalence” is approximate, not exact
- Clinical response matters more than calculations
- Buprenorphine works by stabilizing receptors, not matching euphoria
- Harm reduction is not compromise—it is evidence-based care
📍 About the Author
Evidence-based opioid dependence treatment, including buprenorphine-based OST, is available.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808