From Tramadol to Buprenorphine: A Practical Guide to Opioid Substitution Therapy in India
 Opioid dependence is often imagined in the context of heroin or injectable drug use. Yet, in everyday clinical practice across India, one of the most common—and underestimated—drivers of dependence is Tramadol.
Opioid dependence is often imagined in the context of heroin or injectable drug use. Yet, in everyday clinical practice across India, one of the most common—and underestimated—drivers of dependence is Tramadol.
Patients frequently present with prolonged use, escalating doses, and a failed attempt at “self-detoxification.” The turning point in treatment is often the transition to Buprenorphine, a cornerstone of Opioid Substitution Therapy (OST).
This article explores that transition in depth—scientifically, clinically, and pragmatically.
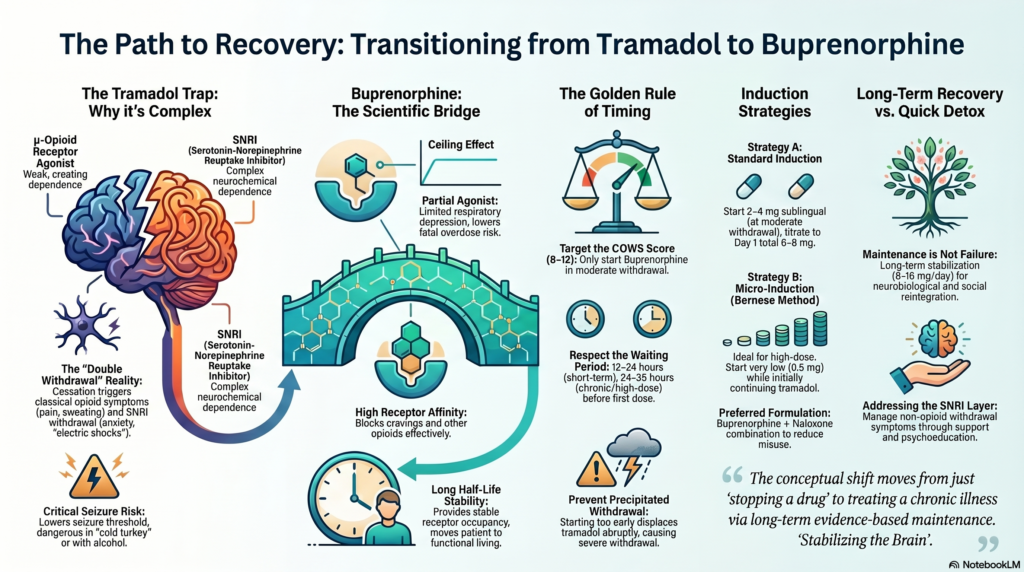
🔹 The Tramadol Problem: Why It Is Not a “Mild Opioid”
Tramadol occupies a unique position in psychopharmacology.
Unlike classical opioids, it has a dual mechanism:
- Weak μ-opioid receptor agonism
- Inhibition of serotonin and norepinephrine reuptake
This dual action creates a false sense of safety. Patients often perceive tramadol as:
- “Less addictive”
- “Safer than other opioids”
- “Easy to stop”
Clinically, the opposite is often true.
The Dependence Pattern
With prolonged use:
- Tolerance develops rapidly
- Doses escalate beyond prescribed limits
- Psychological dependence becomes entrenched
The Withdrawal Complexity
Stopping tramadol is not a simple opioid withdrawal. It includes:
- Classical opioid symptoms (body pain, diarrhea, sweating)
- SNRI discontinuation features:
- Anxiety
- Dysphoria
- “Electric shock” sensations
- Irritability
Most importantly, seizures can occur, particularly at high doses or abrupt cessation.
👉 This is why “cold turkey” is not just ineffective—it can be dangerous.
🔹 Why Buprenorphine? The Science of a Safer Opioid
Buprenorphine represents a paradigm shift in addiction treatment.
Pharmacological Advantages
- Partial agonist at μ-opioid receptors
- Ceiling effect → markedly lower overdose risk
- Long half-life → stable receptor occupancy
- Reduces cravings and withdrawal
Harm Reduction Perspective
Programs across India, including those guided by National Drug Dependence Treatment Centre and National AIDS Control Organisation, recognize buprenorphine as:
- A life-saving intervention
- A tool for functional recovery, not just detoxification
🔹 The Core Clinical Challenge: Transitioning Safely
The transition from tramadol to buprenorphine is not straightforward.
The key risk:
👉 Precipitated withdrawal
This occurs because:
- Buprenorphine has higher receptor affinity
- It displaces tramadol
- But activates the receptor only partially
Result: sudden worsening of withdrawal symptoms
🔹 When to Start Buprenorphine
Timing is everything.
Clinical Rule
Start only when the patient is in moderate withdrawal
- Clinical tool: COWS (Clinical Opiate Withdrawal Scale)
- Target: Score ≥ 8–12
Typical Waiting Period
- Short-term tramadol use: 12–24 hours
- Chronic/high-dose use: 24–36 hours
Rushing this step is the most common cause of treatment failure.
🔹 Two Practical Transition Strategies
1. Standard Induction (Most Common)
Once moderate withdrawal begins:
Day 1
- Start: 2–4 mg sublingual buprenorphine
- Reassess after 1–2 hours
- Repeat dosing if needed
Typical Day 1 total:
- 6–8 mg
Day 2–3
- Stabilize at:
- 8–12 mg/day
2. Micro-Induction (Bernese Method)
An underutilized but highly effective strategy.
When to Consider
- High-dose tramadol dependence
- Severe withdrawal anxiety
- Previous failed attempts
Approach
- Start very low-dose buprenorphine (e.g., 0.5 mg)
- Continue tramadol initially
- Gradually increase buprenorphine
- Stop tramadol over 5–7 days
👉 Advantage:
- Avoids precipitated withdrawal
- Smooth, patient-friendly transitio
🔹 Managing the “Double Withdrawal”
Tramadol withdrawal has two layers:
Opioid Withdrawal
- Managed effectively by buprenorphine
SNRI Discontinuation
Often overlooked, but clinically significant.
Symptoms:
- Anxiety
- Dysphoria
- Irritability
Management:
- Short-term pharmacological support
- Reassurance and psychoeducation
🔹 Seizure Risk: A Critical Consideration
Tramadol lowers seizure threshold.
Risk factors:
- High doses
- Rapid discontinuation
- Comorbid alcohol use
Clinical approach:
- Identify high-risk patients
- Consider short-term:
- Benzodiazepine cover
- Mood stabilizers (select cases)
🔹 Maintenance Phase: Beyond Detoxification
Buprenorphine is not just for withdrawal—it is long-term treatment.
Typical Dose
- 8–16 mg/day
Goals
- Eliminate cravings
- Prevent relapse
- Restore daily functioning
Preferred Formulation
- Buprenorphine + naloxone (sublingual)
Why?
- Reduces misuse potential
- Standard of care globally
🔹 Common Mistakes in Practice
- Starting buprenorphine too early
- Underdosing → persistent cravings
- Ignoring SNRI withdrawal features
- Overemphasis on detox instead of maintenance
- Lack of psychosocial intervention
🔹 A Shift in Perspective: From Detox to Recovery
The most important conceptual shift is this:
👉 Addiction treatment is not about stopping a drug—it is about stabilizing the brain.
Buprenorphine allows:
- Neurobiological stabilization
- Psychological recovery
- Social reintegration
It is not “replacing one addiction with another.”
It is evidence-based treatment for a chronic illness.
🔹 Final Takeaway
If you remember just three points:
- Tramadol dependence is real and complex
- Timing of buprenorphine initiation is critical
- Long-term maintenance is often necessary—not failure
📍 Consultation & Treatment Support
If you or a loved one is struggling with opioid or tramadol dependence, evidence-based treatment is available.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808