Autism Spectrum Condition (ASC) vs Autism Spectrum Disorder (ASD): Why the Words Matter
 Terminology in autism is not just a cosmetic issue. It shapes how a child is seen by parents, how an adult understands their life story, how teachers respond to behaviour, how clinicians formulate distress, and how society decides whether to offer support or judgement.
Terminology in autism is not just a cosmetic issue. It shapes how a child is seen by parents, how an adult understands their life story, how teachers respond to behaviour, how clinicians formulate distress, and how society decides whether to offer support or judgement.
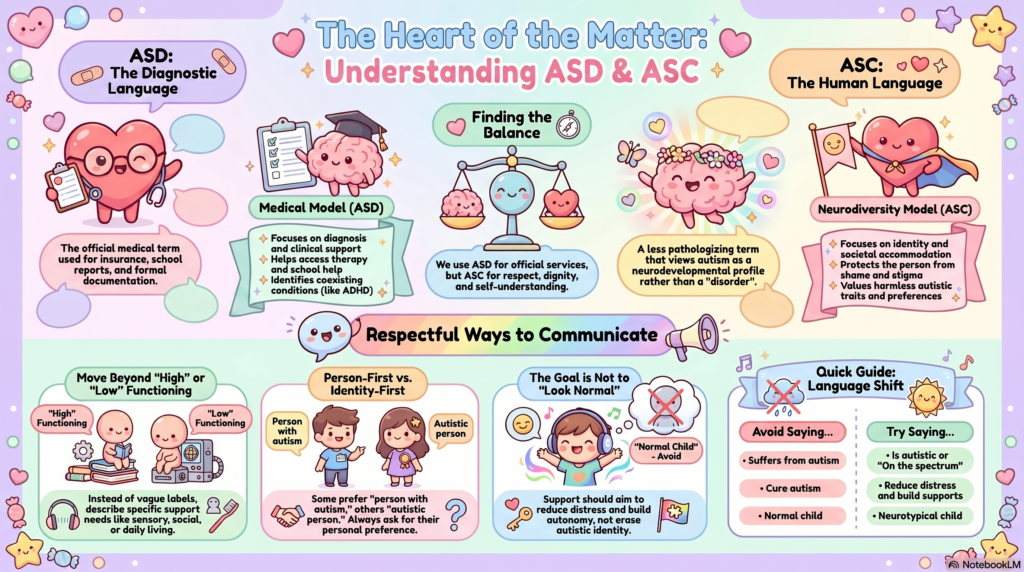
The formal diagnostic term remains Autism Spectrum Disorder — ASD. DSM-5 and DSM-5-TR use ASD as the official term, bringing older labels such as autistic disorder and Asperger’s disorder under one spectrum diagnosis. DSM-5 criteria focus on persistent differences or difficulties in social communication and interaction, along with restricted, repetitive behaviours, sensory features, routines, or interests. ICD-11 also uses Autism Spectrum Disorder as the diagnostic category.
But many clinicians, autistic people, families, and advocates increasingly use Autism Spectrum Condition — ASC in explanation because it feels less pathologising. Autism-Europe notes that some people prefer “autism spectrum condition” or “on the autism spectrum” because these avoid the negative connotations of “disorder.”
The nuance is this: ASD is the diagnostic language; ASC is often the human language.
Why “Disorder” Can Hurt
The word disorder can be useful in medicine because it signals that a clinically recognisable pattern exists, that the person may need support, and that services can be justified. But emotionally, the word can sound like:
“Something is wrong with me.”
For a child, it may create shame.
For parents, it may create fear.
For an adult receiving a late diagnosis, it may feel like a lifelong identity has been reduced to pathology.
This is especially important in people who have spent years masking, being misunderstood, or being labelled as rude, lazy, arrogant, stubborn, emotionally immature, narcissistic, anxious, obsessive, or “difficult.” A respectful diagnostic explanation can convert shame into self-understanding.
Instead of saying:
“You have a disorder.”
A more therapeutic explanation would be:
“Your brain processes social cues, sensory input, predictability, emotions, and communication differently. Some of these differences create strengths; some create distress or disability. Our job is to understand the profile and build the right supports.”
That single shift can change the entire emotional experience of diagnosis.
Why “Condition” Is Not the Same as Minimising Autism
There is a danger on the other side too. If we use only soft language, we may accidentally minimise real suffering.
Autism is not merely a “personality type.” It is not just introversion. It is not just being intelligent, socially awkward, or liking routines. The World Health Organization describes autism as a diverse group of conditions related to brain development, with abilities and needs that vary and may change over time; some autistic people live independently, while others have severe disabilities and require lifelong care and support.
So, ASC should not be used to deny disability.
Some autistic people have major communication challenges, intellectual disability, epilepsy, severe sensory distress, self-injurious behaviour, feeding difficulties, sleep problems, school refusal, shutdowns, meltdowns, or extreme functional impairment. Families may experience real caregiver burden. In such situations, overly romantic language can become invalidating.
The correct position is not:
“Autism is not a disorder, it is only a difference.”
The more balanced position is:
“Autism is a neurodevelopmental condition that may be disabling depending on the person, environment, supports, and coexisting conditions.”
That is both respectful and clinically honest.
The Medical Model and Neurodiversity Model Can Coexist
The debate often becomes unnecessarily polarised.
The medical model says:
There are symptoms, impairments, comorbidities, and support needs that require diagnosis and treatment.
The neurodiversity model says:
Autism is part of natural human brain variation; society should accommodate differences instead of forcing everyone into a narrow idea of normality.
A good clinician should not choose one and reject the other. Both are needed.
The medical model helps us identify ADHD, anxiety, depression, OCD, sleep disorders, epilepsy, intellectual disability, language disorder, trauma, or behavioural crisis. It helps families access services, therapy, school accommodations, disability certification, and structured interventions.
The neurodiversity model protects the person from shame. It reminds us that therapy should not aim to erase harmless autistic traits, suppress identity, or force artificial normality.
The goal is not to make the autistic person “look normal.”
The goal is to reduce distress, improve functioning, build autonomy, and create a better person-environment fit.
Why This Matters in Clinical Practice
Terminology changes the treatment goal.
If we think only in terms of “disorder,” treatment may become:
“Reduce autistic behaviour.”
But if we think in terms of “condition,” treatment becomes:
“Understand the autistic profile and reduce suffering.”
That means we do not automatically target every repetitive behaviour, special interest, routine, or social difference. We ask:
Is this behaviour harmful?
Is it distressing to the person?
Is it interfering with learning, safety, relationships, or independence?
Or is it a self-regulation strategy that others simply do not understand?
For example, hand-flapping, intense interests, avoiding eye contact, needing routines, or preferring written communication may not need “correction.” But severe anxiety, aggression due to sensory overload, self-injury, depression, sleep reversal, school refusal, or caregiver exhaustion definitely need intervention.
This is where language becomes clinical wisdom.
The Problem With “High-Functioning” and “Low-Functioning”
Another reason terminology matters is that older labels can mislead.
Calling someone high-functioning may hide their suffering. A bright adult with a job may still have severe sensory overload, relationship breakdowns, burnout, suicidal thoughts, executive dysfunction, or inability to manage daily living.
Calling someone low-functioning may hide their abilities. A non-speaking autistic person may still understand deeply, communicate through alternative methods, and have preferences, emotions, humour, and intelligence that are underestimated.
A better approach is to describe support needs by domain:
Social communication support
Sensory regulation support
Daily living support
Academic or occupational support
Emotional regulation support
Language and communication support
Behavioural and safety support
Family and caregiver support
This is more clinically useful than a vague label.
“Autistic Person” vs “Person With Autism”
This is another area where clinicians must be careful.
Some prefer person-first language: “person with autism.”
The intention is to emphasise personhood before diagnosis.
Others prefer identity-first language: “autistic person.”
The reason is that autism is not seen as an external disease but as an integral part of perception, identity, and experience.
Research has found that many autistic adults prefer identity-first language, while professionals are more likely to use person-first language. Another large study also found an overall preference for identity-first language among autistic adults.
The best clinical rule is simple:
Ask the person what they prefer.
For children, ask the family, but as the child grows older, ask the child or adolescent directly. Language should not be imposed in the name of respect.
Indian Context: Why ASD Still Matters Officially
In India, formal documents often need the recognised diagnostic term. The Rights of Persons with Disabilities Act uses the term autism spectrum disorder and defines it as a neuro-developmental condition affecting communication, relationships, and behaviour. Therefore, for school reports, disability certification, official letters, insurance, medico-legal documentation, academic research, and hospital records, ASD remains important.
So the practical Indian approach can be:
In diagnosis and documentation:
Autism Spectrum Disorder, as per DSM-5/ICD-11 criteria.
In counselling and psychoeducation:
Autism Spectrum Condition, autism spectrum profile, or autistic neurodevelopmental profile.
In conversation with the person:
Use the term they prefer.
This avoids both extremes: it does not pathologise identity, and it does not weaken access to services.
A More Nuanced Clinical Explanation
A good explanation to a family could be:
“The formal diagnosis is Autism Spectrum Disorder. That is the term used in medical classification and official documents. But I would like you to understand it as an Autism Spectrum Condition — a lifelong neurodevelopmental profile. It affects social communication, sensory processing, flexibility, emotional regulation, routines, and interests. Some aspects may be strengths. Some may cause distress or disability. Our goal is not to change the person’s nature, but to reduce distress, treat coexisting problems, improve functioning, and help the environment understand the person better.”
This explanation is accurate, compassionate, and practical.
What We Should Avoid Saying
Avoid:
“Suffers from autism”
“Victim of autism”
“Normal child” versus “autistic child”
“Mild autism, so no problem”
“Severe autism, so no potential”
“Autism disease”
“Cure autism”
“Just poor parenting”
“Just screen addiction”
“Just stubborn behaviour”
Autism-Europe specifically recommends avoiding expressions like “suffers from” or “victim of autism,” and suggests alternatives such as “is autistic,” “on the autism spectrum,” or “has autism / ASD / ASC.”
The Real Purpose of Diagnosis
Diagnosis should not become a label that limits the person.
A good autism assessment should answer:
What is the person’s developmental profile?
What are their strengths?
Where do they need support?
Are there coexisting conditions like ADHD, anxiety, depression, OCD, sleep problems, intellectual disability, language disorder, trauma, or epilepsy?
What changes are needed at home, school, college, workplace, or relationships?
What should not be unnecessarily treated?
What must be actively treated?
That is why terminology matters. Words decide whether autism becomes a verdict or a map.
Bottom Line
ASD is necessary for diagnosis, research, documentation, and services.
ASC is often better for psychoeducation, dignity, and identity.
Neither term is perfect. The best clinicians use language flexibly, respectfully, and precisely.
Autism is not simply a disorder to be removed.
It is not merely a difference to be romanticised.
It is a neurodevelopmental condition with a highly individual profile of strengths, vulnerabilities, distress, disability, and support needs.
The right language does not dilute science.
It makes science humane.
For Autism, ADHD, and Neurodevelopmental Assessment in Chennai
At Mind & Memory Clinic, Apollo Clinic Velachery, I provide detailed psychiatric assessment for children, adolescents, and adults with suspected Autism Spectrum Disorder/Condition, ADHD, anxiety, emotional dysregulation, OCD traits, sensory issues, social communication difficulties, and complex overlapping presentations.
The focus is on careful clinical evaluation, developmental history, comorbidity assessment, psychoeducation, family guidance, and a practical support plan rather than simply giving a label.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery, Chennai
✉ srinivasaiims@gmail.com
📞 +91-8595155808