When the Body Keeps the Score: Can Narcosynthesis Help the Silent Mind Heal?
 Introduction
Introduction
The phrase “the body keeps the score” has become one of the most powerful ways to understand trauma, anxiety, dissociation, and emotional shutdown.
Many people assume trauma is stored only as a memory.
But clinically, trauma often appears first in the body.
A person may say, “I have moved on.”
But the body may still react as if the danger is happening now.
The heart races.
The throat tightens.
The body freezes.
The voice disappears.
The mind goes blank.
Sleep becomes disturbed.
Pain appears without a clear medical explanation.
The person avoids people, places, intimacy, conflict, or silence.
This is where the older psychiatric idea of narcosynthesis becomes interesting again.
Not as a “truth serum.”
Not as forced memory recovery.
Not as dramatic catharsis.
But as a way of understanding how psychiatry can help a frozen mind and body slowly find words, safety, and meaning.
What does “the body keeps the score” mean?
When a person goes through overwhelming fear, humiliation, helplessness, abuse, loss, violence, or emotional neglect, the brain may not process the event as an ordinary memory.
Ordinary memory says:
“This happened in the past.”
Traumatic memory often says:
“This is still happening.”
That is why trauma can return as:
- panic attacks,
- nightmares,
- flashbacks,
- body pain,
- choking sensation,
- trembling,
- numbness,
- dissociation,
- irritability,
- emotional shutdown,
- avoidance,
- unexplained fatigue,
- or inability to speak.
The body remembers before the mind explains.
A smell, tone of voice, facial expression, room, argument, or touch may trigger a reaction that feels disproportionate to the present situation.
But the reaction is not random.
The nervous system is responding to an old danger signal.
Trauma is not only remembered. It is re-lived.
In many patients, trauma does not come as a clean story.
It comes as fragments.
A sensation.
A fear.
A blankness.
A pain.
A startle response.
A collapse.
A sudden anger.
A feeling of being trapped.
A body that refuses to move.
A voice that refuses to come out.
This is why some people struggle to explain their distress.
They may say:
“I don’t know why I react like this.”
“My body shuts down.”
“I freeze.”
“I cannot speak.”
“I know I am safe, but I don’t feel safe.”
“I feel like something bad is going to happen.”
“I don’t remember clearly, but my body reacts.”
This is the clinical space where psychiatry must move beyond symptom labels.
The deeper question is:
What is the body trying to say that the mind cannot yet put into words?
What is narcosynthesis?
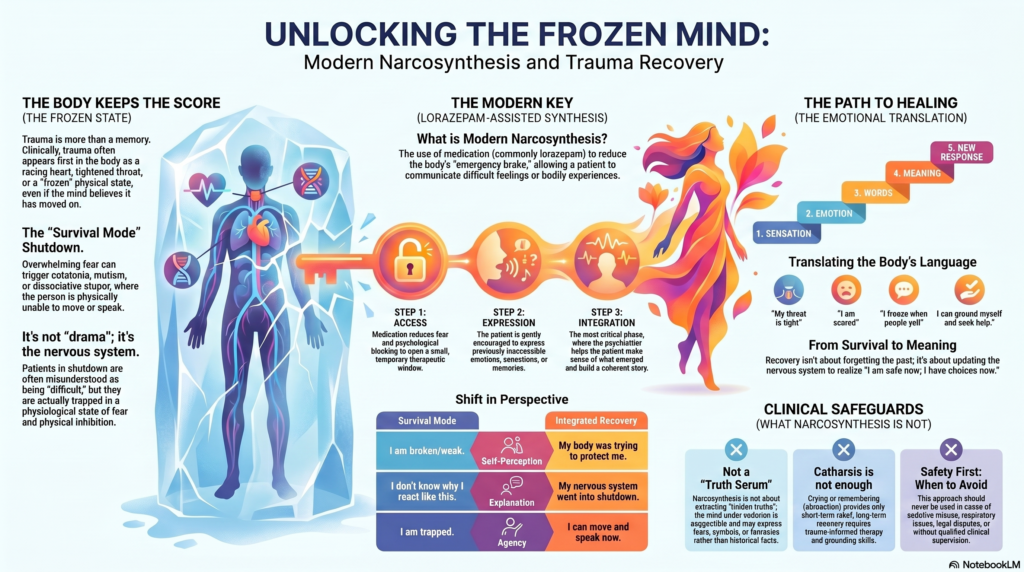
Narcosynthesis is a historical psychiatric technique in which sedative medication was used to reduce inhibition, anxiety, mutism, or emotional blocking so that the patient could communicate difficult memories, feelings, or conflicts.
Classically, drugs such as sodium Amytal were used.
But the important point is this: narcosynthesis was never meant to be merely drug-induced talking.
It had three stages:
1. Access
The medication reduced fear, inhibition, mutism, or psychological blocking.
2. Expression
The patient could express previously inaccessible emotions, memories, or bodily experiences.
3. Integration
The psychiatrist helped the patient make sense of what emerged.
The third stage is the most important.
Without integration, it is only catharsis.
With integration, it becomes therapy.
The older Amytal interview literature clearly noted that such techniques had limited usefulness, were not specific for any psychiatric disorder, and were valuable only in carefully selected cases. It also cautioned that material emerging during such interviews should not be treated as automatic truth.
Narcosynthesis is not “truth serum psychiatry”
One of the biggest myths about narcosynthesis is that it can uncover the exact truth.
That is not correct.
The mind under sedation may become more expressive, but it may also become more suggestible.
What emerges may include:
- real memories,
- emotional truths,
- symbolic material,
- fears,
- fantasies,
- body memories,
- shame,
- guilt,
- confusion,
- or therapist-influenced responses.
Therefore, modern psychiatry must be careful.
The aim is not to ask:
“What really happened?”
The better question is:
“What is the patient experiencing, feeling, fearing, and carrying?”
This distinction matters.
A memory may be historically accurate.
A feeling may be emotionally true.
A body response may be clinically meaningful.
But all three are not the same thing.
Good psychiatry respects this complexity.
The modern version: Lorazepam-assisted synthesis
Today, sodium Amytal is rarely used in routine psychiatry.
But the idea behind narcosynthesis can be reimagined using safer and more familiar medication such as lorazepam, especially in selected cases.
Lorazepam is commonly used in psychiatry for acute anxiety, agitation, insomnia, alcohol withdrawal, and catatonia. In catatonia, it can sometimes produce striking improvement.
A patient who was mute may begin to speak.
A patient who was frozen may begin to move.
A patient who refused food may accept fluids.
A patient who looked unreachable may become emotionally available.
This is not because lorazepam reveals hidden truth.
It may temporarily reduce the body’s emergency brake.
It may create a small therapeutic window.
That window must be used gently, ethically, and clinically.
When the body freezes: catatonia, dissociation, and trauma shutdown
Some psychiatric states are not simply “mental.”
They are whole-body states.
In catatonia, the patient may appear motionless, mute, rigid, withdrawn, or negativistic.
In dissociation, the patient may appear present but internally disconnected.
In trauma shutdown, the patient may freeze, go blank, collapse, or become unable to speak.
In functional neurological symptoms, the body may express distress through weakness, tremors, paralysis-like states, seizures, pain, or sensory symptoms without a structural neurological explanation.
In such states, the patient is often misunderstood.
Families may say:
“She is acting.”
“He is stubborn.”
“She is doing it deliberately.”
“He just doesn’t want to talk.”
“She is attention-seeking.”
But clinically, the person may be trapped in a nervous system state of fear, inhibition, or shutdown.
This is where a modern narcosynthesis-inspired approach becomes useful.
Not to expose the patient.
But to understand the patient.
How lorazepam may help the silent mind speak
In selected cases, lorazepam may reduce overwhelming anxiety, motor inhibition, or catatonic blocking.
Once the patient becomes calmer or more communicative, the psychiatrist can gently explore the inner experience.
The questions must be careful:
“What are you feeling now?”
“What was happening inside when you could not speak?”
“Were you afraid?”
“Did your body feel stuck?”
“Did something trigger this?”
“Did you feel unsafe?”
“What helped you feel calmer now?”
“What should we understand about your experience?”
The aim is not memory excavation.
The aim is emotional translation.
The patient begins to move from:
“I don’t know what happened”
to
“My body froze when I felt unsafe.”
From:
“I am weak”
to
“My nervous system went into shutdown.”
From:
“I was pretending”
to
“My symptoms were real, but treatable.”
From:
“I am broken”
to
“My body was trying to protect me.”
That is synthesis.
How can you escape when the body keeps the score?
You do not escape by fighting the body.
You escape by helping the body learn safety again.
Trauma recovery is not about forcing the body to forget.
It is about teaching the nervous system:
“The danger is over.”
“I am safe now.”
“I have choices now.”
“I can speak now.”
“I can move now.”
“I can protect myself now.”
“I am no longer trapped in the past.”
The escape route is not suppression.
It is integration.
The healing movement is:
Sensation → emotion → words → meaning → new response
For example:
“I feel tightness in my throat.”
becomes
“I am scared.”
becomes
“I freeze when someone raises their voice.”
becomes
“My body learnt this from earlier helplessness.”
becomes
“I can ground myself, step away, speak, seek help, and recover.”
This is how the body slowly updates its score.
Why catharsis alone is not enough
Many people think healing means crying, remembering, or releasing emotion.
That may help briefly.
But catharsis alone is not enough.
The older Amytal literature itself recognised that simple abreaction may produce short-term relief, but long-term improvement is uncertain unless the material is integrated through psychotherapy.
A patient may cry intensely and still relapse.
A patient may remember something and still remain symptomatic.
A patient may speak after lorazepam and still need long-term care.
The real treatment begins after the dramatic moment.
The patient needs:
- psychoeducation,
- diagnosis,
- grounding skills,
- family understanding,
- sleep restoration,
- trauma-informed therapy,
- treatment of depression or anxiety,
- treatment of catatonia where present,
- relapse prevention,
- and a safe therapeutic relationship.
The goal is not one emotional breakthrough.
The goal is durable recovery.
Buried memories: handle with care
The phrase “buried memories” is attractive and SEO-friendly, but clinically it must be used with caution.
Not every symptom is due to a hidden memory.
Not every recovered memory is accurate.
Not every emotional reaction needs excavation.
Sometimes the body is not hiding a secret.
It is expressing a pattern.
The psychiatrist’s task is not to force memory.
The task is to help the patient develop a coherent, safe, and compassionate understanding of their symptoms.
The best clinical question is not:
“What memory is buried?”
The better question is:
“What experience is unprocessed?”
That experience may be a memory.
It may be grief.
It may be shame.
It may be fear.
It may be chronic invalidation.
It may be emotional neglect.
It may be a body state that never found words.
A modern clinical example
A young woman is brought to the clinic after suddenly becoming mute and immobile following a severe family conflict.
The family says, “She is doing drama.”
On examination, she appears frozen, fearful, and unable to respond. Catatonia or dissociative shutdown is considered.
In a supervised clinical setting, lorazepam is given. After some time, she begins to speak softly.
The wrong approach would be:
“Now tell us the truth.”
The right approach would be:
“You seem a little safer now. Can you tell me what was happening inside when you could not speak?”
She says:
“I felt trapped. I wanted to speak, but my body would not allow me.”
This single sentence changes the family’s understanding.
She was not acting.
She was frozen.
The psychiatrist can now explain:
“Her nervous system entered a shutdown state. Medication helped unlock the block temporarily. Now we must understand the stress, treat the underlying condition, and help her body and mind recover safely.”
This is modern narcosynthesis.
Not confession.
Not spectacle.
Not magic.
A careful movement from silence to story.
Where this approach may be useful
A narcosynthesis-inspired, lorazepam-assisted approach may be considered in selected cases of:
- catatonia,
- severe anxiety shutdown,
- psychogenic mutism,
- dissociative stupor,
- trauma-related freezing,
- acute grief with shutdown,
- functional neurological symptoms,
- severe panic with inability to communicate.
It must be used cautiously and only by qualified clinicians.
It is not suitable for casual use, self-medication, or forced disclosure.
When it should be avoided
This approach may be risky or inappropriate in:
- alcohol intoxication,
- sedative misuse,
- opioid use,
- respiratory compromise,
- obstructive sleep apnoea,
- severe medical instability,
- delirium,
- elderly frailty,
- pregnancy without proper evaluation,
- severe paranoia,
- active coercive family situations,
- legal disputes,
- unrealistic expectation of “truth extraction.”
The patient’s dignity and safety must always come first.
Narcosynthesis and psychotherapy
Medication may open the door.
Psychotherapy helps the patient walk through it.
After the initial unlocking, therapy helps the patient:
- understand triggers,
- name body sensations,
- regulate emotions,
- reduce avoidance,
- rebuild trust,
- process trauma safely,
- improve self-compassion,
- and create a new life narrative.
The most important message to the patient is:
“You were not weak. Your body was trying to survive. Now we can help it learn a safer way.”
The real escape: from survival mode to meaning
When the body keeps the score, the person remains trapped in survival mode.
The body keeps asking:
“Am I safe?”
“Will it happen again?”
“Can I trust?”
“Can I speak?”
“Can I move?”
“Can I rest?”
Healing happens when the answer slowly becomes:
“Yes, I am safe enough now.”
“Yes, I can speak now.”
“Yes, I can feel without collapsing.”
“Yes, I can remember without being destroyed.”
“Yes, I can live beyond what happened.”
That is the deepest form of recovery.
Not forgetting.
Not suppressing.
Not forcing memory.
But integrating the past so it no longer controls the present.
Conclusion
When the body keeps the score, the mind may go silent.
Narcosynthesis, in its modern reimagined form, reminds us that some psychiatric symptoms are not deliberate, fake, or attention-seeking. They may be expressions of a nervous system frozen by fear, trauma, dissociation, or catatonia.
Lorazepam may sometimes create a temporary window where speech, movement, and emotional access return. But the medication is only the beginning.
The real healing lies in what follows:
careful listening, correct diagnosis, family education, psychotherapy, body-based regulation, and compassionate integration.
The goal is not to dig out buried memories by force.
The goal is to help the silent body finally feel safe enough to speak.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
Related posts:
- The Body Keeps the Score: Exploring Trauma Science and the Debate on Neuroscience
- Unlocking the Silent Mind: Narcosynthesis Reimagined with Lorazepam
- mECT: A Safe and Scientific Way to Heal the Mind
- Exercise and ADHD: Moving the Body, Calming the Mind
- Myndlift for Anxiety: Can Home-Based Neurofeedback Help Calm the Mind?
- The Mind and Heart Diets – DASH, MIND, and Mediterranean