The Fate of Delusions: Evolution, Transformation, and Resolution in Psychopathology
 Introduction: Do Delusions End—or Do They Transform?
Introduction: Do Delusions End—or Do They Transform?
In clinical psychiatry, we often ask:
- How do delusions form?
- How do we treat them?
But a quieter, deeper question remains:
What happens to a delusion over time?
Does it:
- Disappear?
- Persist unchanged?
- Transform into something else?
The answer, as clinical experience repeatedly shows, is that delusions rarely “end” abruptly.
They have a trajectory—a fate shaped by biology, meaning, and relationship.
Delusion as Experience: The Starting Point of Its Fate
Any discussion of outcome must begin with its nature.
As emphasized in classical psychopathology:
“Phenomenologically it is an experience.”
And:
“The primary delusional experience is… not considered interpretations but meaning directly experienced.”
This has profound implications:
👉 A delusion is not merely a thought to be erased
👉 It is an altered mode of reality-experience
Therefore, its fate is not simple disappearance—but reorganization of experience
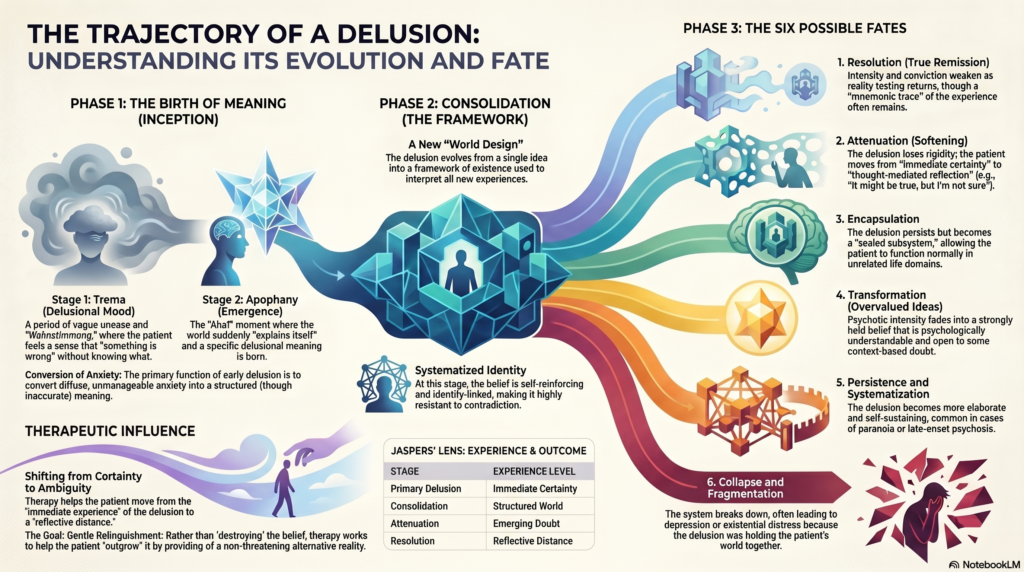
Early Phase: The Birth of Meaning
Before a delusion becomes fixed, it passes through stages.
Klaus Conrad described:
1. Trema (Delusional Mood / Wahnstimmung)
- Vague unease
- Sense that “something is wrong”
2. Apophany
- Sudden emergence of meaning
- The world “explains itself”
At this stage, the delusion serves a crucial function:
It converts diffuse anxiety into structured meaning
Consolidation: The Delusion as a Stable World
Once formed, the delusion becomes:
- Systematized
- Identity-linked
- Self-reinforcing
The patient begins to:
- Interpret all experiences through it
- Act in accordance with it
This corresponds to what Conrad described as consolidation—a new “world design.”
At this stage, the delusion is no longer just an idea:
👉 It is a framework of existence
Possible Fates of Delusions
The longitudinal course of delusions can take several paths.
1. Resolution (True Remission)
In some cases—especially acute psychosis:
- Delusional intensity decreases
- Conviction weakens
- Reality testing returns
This may occur through:
- Antipsychotic treatment
- Natural course
- Restoration of neurobiological balance
Yet even here, remnants may persist:
- “I know it wasn’t real… but it felt real.”
👉 The experience leaves a mnemonic and emotional trace
2. Attenuation (Softening Without Disappearance)
More commonly, delusions do not vanish but:
- Lose rigidity
- Become less central
- Are held with partial doubt
This reflects a shift from:
- Unmittelbar (immediate certainty)
to - Gedanklich vermittelt (thought-mediated reflection)
The patient may say:
- “It might be true… but I’m not sure.”
👉 This is one of the most meaningful therapeutic outcomes
3. Encapsulation
In chronic conditions, delusions may:
- Persist
- But become circumscribed
The patient:
- Maintains belief in specific domains
- Functions relatively normally otherwise
This is often seen in:
- Delusional disorder
- Chronic schizophrenia
👉 The delusion becomes a sealed subsystem within the psyche
4. Transformation into Overvalued Ideas
With time, some delusions:
- Lose their psychotic intensity
- Become overvalued ideas
That is:
- Still strongly held
- But now:
- Open to doubt
- Contextually influenced
This represents a shift from:
- Nicht verstehbar (un-understandable)
to - Verstehbar (psychologically meaningful)
5. Persistence and Systematization
In certain cases, delusions:
- Become more elaborate
- Integrate new experiences
- Resist treatment
This is particularly seen in:
- Paranoia
- Late-onset psychosis
Such delusions:
- Gain internal coherence
- Become resistant to contradiction
👉 They evolve into self-sustaining explanatory systems
6. Collapse and Fragmentation
Occasionally, especially with treatment:
- The delusional system collapses
This may lead to:
- Confusion
- Depression
- Existential distress
Because:
👉 The delusion had been holding the patient’s world together
Psychodynamic Fate: What Lies Beneath
Sigmund Freud famously observed:
“The delusion is… an attempt at recovery.”
If so, then its fate depends on whether:
- The underlying conflict is resolved
- Or remains active
Possible outcomes:
- Conflict resolved → delusion fades
- Conflict persists → delusion persists or transforms
Cognitive Fate: Belief Updating vs Rigidity
From a cognitive perspective:
- Delusions persist when:
- Confirmation bias dominates
- Alternative explanations are rejected
They soften when:
- Evidence accumulates
- Cognitive flexibility improves
Neurobiological Fate: Salience Modulation
Dopaminergic models suggest:
- Delusions arise from aberrant salience
Their fate depends on:
- Whether salience attribution normalizes
Antipsychotics:
- Reduce salience
- Allow reinterpretation
Therapeutic Influence on the Fate of Delusions
Therapy does not “remove” delusions directly.
It influences their trajectory.
1. Relationship as Stabilizer
The therapist provides:
- A consistent external reality
- A non-threatening alternative
2. Meaning Reworking
Instead of:
- Challenging belief
Therapy:
- Explores meaning
- Builds alternative narratives
3. Tolerating Uncertainty
The key shift:
- From certainty → ambiguity
This allows:
- Gradual belief revision
A Phenomenological View of Outcome
From a Jaspersian lens, the fate of delusion is a movement:
| Stage | Experience |
|---|---|
| Primary delusion | Immediate certainty |
| Consolidation | Structured world |
| Attenuation | Emerging doubt |
| Resolution | Reflective distance |
The Residuum: What Remains
Even after remission, patients often retain:
- Emotional memory
- Existential insight
- Residual sensitivity
Delusion leaves behind:
👉 A trace of altered reality-experience
Final Conceptual Insight
The fate of delusions is not binary (present vs absent).
It is a process of transformation:
From immediate experience → structured belief → reflective distance → possible reintegration into shared reality.
Conclusion
Delusions do not simply disappear.
They:
- Emerge to solve a crisis
- Stabilize a disturbed world
- And eventually:
- Dissolve
- Transform
- Or persist in modified form
Understanding their fate allows us to:
- Be patient
- Avoid premature confrontation
- Work with—not against—the patient’s experience
Closing Reflection
Perhaps the most humane way to understand the fate of a delusion is this:
It is not something to be destroyed,
but something that must be outgrown, understood, and gently relinquished.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808