Quit Alcohol Forever with Disulfiram: The Indian Family-Supervised Model
 In India, alcohol recovery is rarely an individual journey alone. A patient may suffer alone, but the consequences of alcohol dependence are often carried by the whole family: spouse, parents, children, siblings, workplace, and finances. This is why family-supervised oral disulfiram, used only after detoxification, medical assessment, and informed consent, can be a very practical approach for selected patients.
In India, alcohol recovery is rarely an individual journey alone. A patient may suffer alone, but the consequences of alcohol dependence are often carried by the whole family: spouse, parents, children, siblings, workplace, and finances. This is why family-supervised oral disulfiram, used only after detoxification, medical assessment, and informed consent, can be a very practical approach for selected patients.
Disulfiram is not a “craving tablet.” It is not a sedative. It is not a cure by itself. It is a deterrent medicine that helps a motivated person remain abstinent by making alcohol physically unsafe to consume while the medicine is active. Official prescribing information clearly states that disulfiram is an aid for selected alcohol-dependent patients who want to remain sober so that supportive and psychotherapeutic treatment can work better; it is not a stand-alone cure.
Why disulfiram suits the Indian context
In many Indian families, the patient is not living alone. There may be a spouse, parent, sibling, or responsible adult who is genuinely invested in the patient’s recovery. This can become a strength.
The biggest practical problem with disulfiram is not the tablet itself. It is adherence. A patient may take disulfiram sincerely for a few days, then stop it quietly before a planned drinking episode. Family supervision prevents this silent stopping.
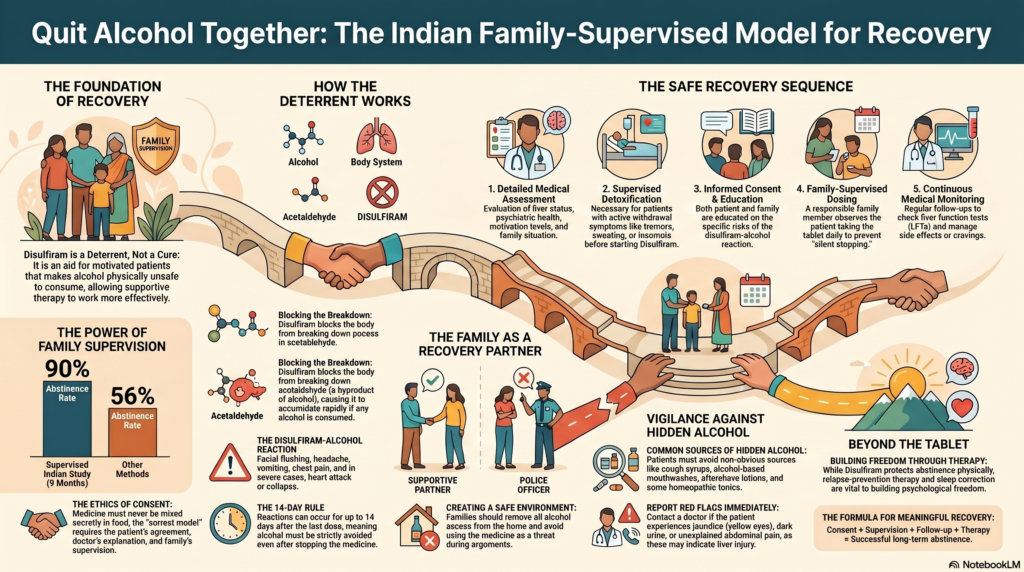
An Indian randomized study comparing disulfiram and topiramate in routine clinical practice included alcohol-dependent men whose family members agreed to encourage compliance and accompany them for follow-up. In that study, family support was used to maintain compliance, and at 9 months, abstinence was reported in 90% of disulfiram patients compared with 56% of topiramate patients.
This does not mean disulfiram is best for everyone. It means that when the patient is motivated and the family supervises treatment ethically, disulfiram can be very effective.
The key principle: consent first
Disulfiram should never be mixed secretly in food, tea, coffee, or juice without the patient’s knowledge.
This is especially important in India, where some families may ask for a “reaction tablet” to be given without telling the patient. That is unsafe and unethical. Disulfiram prescribing information clearly warns that it should never be given when the patient is intoxicated or without the patient’s full knowledge, and relatives must be instructed accordingly.
The correct model is:
Patient agrees. Doctor explains. Family supervises. Everyone knows the risks.
Family supervision should be supportive, not punitive. The family member is not a police officer. They are a recovery partner.
How disulfiram works
When alcohol is consumed, the body converts it into acetaldehyde and then breaks acetaldehyde down further. Disulfiram blocks this second step. As a result, acetaldehyde accumulates in the body if alcohol is consumed. This causes the disulfiram-alcohol reaction.
This reaction may include:
| Symptoms after drinking on disulfiram |
|---|
| Facial flushing |
| Headache |
| Nausea and vomiting |
| Sweating |
| Palpitations |
| Chest pain |
| Breathlessness |
| Dizziness |
| Low blood pressure |
| Fainting |
| Confusion |
| In severe cases: arrhythmia, collapse, seizure, heart attack, or death |
This is why the patient must understand one simple rule:
If you are taking disulfiram, alcohol is not an option.
When should disulfiram be started?
Disulfiram should not be started while the patient is drunk, withdrawing severely, or still ambivalent about drinking.
A safe sequence is:
- Detailed assessment
Drinking pattern, withdrawal risk, liver status, psychiatric comorbidity, suicidality, family situation, and motivation are assessed. - Detoxification if needed
Patients with tremors, sweating, insomnia, seizures, confusion, or morning drinking may need supervised detoxification before relapse-prevention medication. - Baseline medical checks
Liver function tests are important. ECG may be needed in older patients or those with cardiac risk. - Informed consent
The patient and family are educated about the disulfiram-alcohol reaction. - Family-supervised oral tablet
A responsible family member watches the patient take the medicine as prescribed. - Regular follow-up
Review is needed for side effects, liver safety, cravings, mood, sleep, and relapse risk.
Disulfiram administration should not begin until the patient has abstained from alcohol for at least 12 hours, and patients are usually advised to avoid alcohol-containing products even after stopping disulfiram because reactions can occur for up to 14 days.
Who is suitable for family-supervised disulfiram?
Disulfiram works best when the patient says:
“Doctor, I have decided. I do not want controlled drinking. I want complete abstinence.”
Good candidates usually have:
| Suitable patient profile |
|---|
| Clear decision to stop alcohol completely |
| Completed detoxification or no active withdrawal |
| Reliable family member available for supervision |
| Good understanding of risks |
| Willingness for follow-up |
| No severe liver disease |
| No serious heart disease |
| No active psychosis |
| No severe cognitive impairment |
| No ongoing secret alcohol use |
Disulfiram should be used cautiously or avoided in patients with significant cardiac disease, psychosis, severe liver disease, seizures, cognitive impairment, or poor ability to understand the consequences of drinking on the medication.
The family’s role
The family’s role is not to shame, threaten, or control the patient. The family’s role is to help the patient protect a decision made during a clear moment.
A good family-supervised system looks like this:
| Family task | Correct approach |
|---|---|
| Supervise tablet | Watch the patient take it calmly |
| Avoid arguments | Do not use the medicine as a threat |
| Remove alcohol access | No alcohol at home |
| Watch warning signs | Mood change, craving, irritability, sleep disturbance |
| Attend follow-up | Join review when needed |
| Support routine | Meals, sleep, work, exercise |
| Respond early to slips | Contact doctor early, do not hide relapse |
A poor system looks like this:
| Avoid this |
|---|
| Secretly mixing disulfiram |
| Forcing the patient physically |
| Public humiliation |
| Threatening divorce or abandonment repeatedly |
| Using children to monitor the patient |
| Assuming tablet alone is enough |
| Stopping follow-up once drinking stops |
Hidden alcohol: a common Indian problem
Patients must avoid not only liquor, beer, wine, and toddy, but also hidden alcohol sources.
These may include:
| Possible alcohol sources |
|---|
| Some cough syrups |
| Alcohol-based tonics |
| Homeopathic preparations containing alcohol |
| Mouthwashes |
| Aftershave lotions |
| Certain herbal preparations |
| Some fermented preparations |
| Food cooked with alcohol |
| “Just one sip” at social functions |
The prescribing information specifically warns patients to avoid disguised forms of alcohol such as cough mixtures, sauces, vinegar, aftershave lotions, and similar products.
Monitoring and safety
Disulfiram can rarely cause liver injury. Patients should immediately report tiredness, weakness, loss of appetite, nausea, vomiting, jaundice, dark urine, or unexplained abdominal discomfort. Baseline and follow-up liver function monitoring is recommended.
The doctor may monitor:
| Monitoring area | Why it matters |
|---|---|
| Liver function tests | To detect liver injury early |
| Blood pressure | Disulfiram may occasionally affect BP |
| Neuropathy symptoms | Numbness, tingling, weakness |
| Mood and sleep | Depression, anxiety, insomnia can trigger relapse |
| Craving level | May need additional medication or therapy |
| Family stress | Conflict can destabilize recovery |
| Adherence | Supervision prevents silent discontinuation |
Disulfiram is not enough by itself
A patient may stop alcohol physically but still remain psychologically dependent on it. That is why treatment must include relapse prevention.
A complete Indian recovery plan should include:
| Recovery component | Purpose |
|---|---|
| Detoxification | Safe withdrawal from alcohol |
| Disulfiram | External protection against drinking |
| Family supervision | Improves adherence |
| Psychoeducation | Helps patient and family understand addiction |
| Relapse-prevention therapy | Teaches trigger management |
| Sleep correction | Reduces evening vulnerability |
| Treatment of depression/anxiety | Prevents emotional relapse |
| Work and routine rebuilding | Restores dignity and structure |
| Follow-up | Keeps recovery accountable |
Disulfiram protects abstinence. Therapy builds freedom.
A simple consent-based disulfiram contract
Before starting, the patient and family should understand and agree to something like this:
I understand that disulfiram is being prescribed to help me remain abstinent from alcohol.
I understand that drinking alcohol while taking disulfiram can cause a serious reaction.
I agree not to consume alcohol or alcohol-containing products.
I agree that a family member may supervise my tablet intake.
I understand that this medicine is being given with my knowledge and consent.
I will attend follow-up and report side effects early.
I understand that this tablet is only one part of recovery and that counselling, lifestyle change, and relapse-prevention planning are also necessary.
This transforms disulfiram from a “fear tablet” into a shared recovery agreement.
The central message
In the Indian context, family-supervised oral disulfiram can be a powerful and practical tool for alcohol abstinence — but only when used correctly.
The right formula is:
No secret dosing. No coercion. No drinking. No shortcuts.
Consent + supervision + follow-up + therapy = meaningful recovery.
Alcohol dependence is treatable. Many patients who repeatedly failed with willpower alone can recover when treatment is structured, supervised, and compassionate.
Disulfiram does not create recovery by fear alone. It gives the patient time to rebuild a sober life — one supervised morning at a time.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery
Opp. Phoenix Mall, Chennai
✉ srinivasaiims@gmail.com
📞 +91-8595155808
Related posts:
- How to Quit Smoking Forever: A Step-by-Step Guide That Works
- How to Support a Family Member Trying to Quit Smoking
- How to Make a Marriage Last Forever
- Allostasis and Addiction: Why It’s So Hard to Quit Alcohol and Other Substances
- Artificial Alcohol: Acamprosate – The Sober Solution for Alcohol Dependence
- 🌿 Why Quit Cannabis? – Understanding the Harms and Why It’s Worth Letting Go