Frontal Lobe and Its Relevance in Psychiatry
 Frontal Lobe and Its Relevance in Psychiatry Structure, Functional Anatomy, Circuits, and Clinical Disorders
Frontal Lobe and Its Relevance in Psychiatry Structure, Functional Anatomy, Circuits, and Clinical Disorders
The frontal lobe is the most “psychiatric” part of the brain. It is not simply the seat of intelligence; it is the region that helps a person plan, inhibit, choose, delay gratification, regulate emotion, judge social context, shift flexibly, and convert inner intention into purposeful action. Many psychiatric symptoms can be understood as problems of frontal regulation over limbic, striatal, thalamic, and sensory systems.
1. Anatomical Boundaries of the Frontal Lobe
The frontal lobe lies anterior to the central sulcus and superior to the lateral/Sylvian fissure. It is the largest cerebral lobe and includes motor, premotor, supplementary motor, frontal eye field, language-related, and prefrontal association cortices. The prefrontal cortex is the anterior part of the frontal lobe and is central to higher-order cognitive, emotional, and behavioural regulation.
Major landmarks
Posterior boundary
Central sulcus separates frontal lobe from parietal lobe.
Inferior boundary
Lateral/Sylvian fissure separates frontal lobe from temporal lobe.
Medial surface
Includes medial frontal cortex, supplementary motor area, and anterior cingulate cortex.
Inferior/orbital surface
Contains the orbitofrontal cortex, lying above the orbits.
2. Major Structural Divisions
A. Primary Motor Cortex
Brodmann area 4
Located in the precentral gyrus. It controls voluntary movement of the opposite side of the body. The motor homunculus is arranged somatotopically: face and hand laterally, leg medially.
Clinical relevance
Lesions cause contralateral weakness, spasticity, hyperreflexia, and upper motor neuron signs. In psychiatry, this area is less central, but motor slowing, catatonia, psychomotor agitation, and extrapyramidal syndromes interact with frontal-subcortical systems.
B. Premotor Cortex
Lateral BA 6
Involved in planning and sequencing externally guided movements.
Clinical relevance
Dysfunction may contribute to motor disorganization, impaired imitation, apraxia-like phenomena, and poor motor planning.
C. Supplementary Motor Area
Medial BA 6
Involved in internally generated movement, initiation, sequencing, and bimanual coordination.
Clinical relevance
Damage may cause akinesia, reduced spontaneous speech, motor initiation difficulty, or supplementary motor area syndrome. In psychiatry, this region is relevant to catatonia, psychomotor retardation, and volitional impairment.
D. Frontal Eye Field
BA 8
Controls voluntary saccadic eye movements, especially gaze to the opposite side.
Clinical relevance
Important in neurological examination. Abnormalities in eye movements and antisaccade tasks are studied in schizophrenia and frontal executive dysfunction.
E. Broca’s Area
Usually BA 44 and 45 in the dominant inferior frontal gyrus.
Involved in speech production, verbal fluency, syntactic processing, and motor planning of language.
Clinical relevance
Lesions produce non-fluent expressive aphasia. In psychiatry, inferior frontal language networks are relevant to thought disorder, inner speech, verbal hallucinations, and language disorganization in schizophrenia-spectrum disorders.
F. Prefrontal Cortex
The most relevant region for psychiatry.
It includes:
- Dorsolateral prefrontal cortex
- Ventromedial prefrontal cortex
- Orbitofrontal cortex
- Anterior cingulate cortex
- Frontopolar cortex
The prefrontal cortex is heavily connected with limbic structures, basal ganglia, thalamus, parietal association areas, temporal cortex, and brainstem neuromodulatory systems. This makes it a control hub rather than an isolated “thinking centre.”
3. Functional Anatomy of the Prefrontal Cortex
3.1 Dorsolateral Prefrontal Cortex
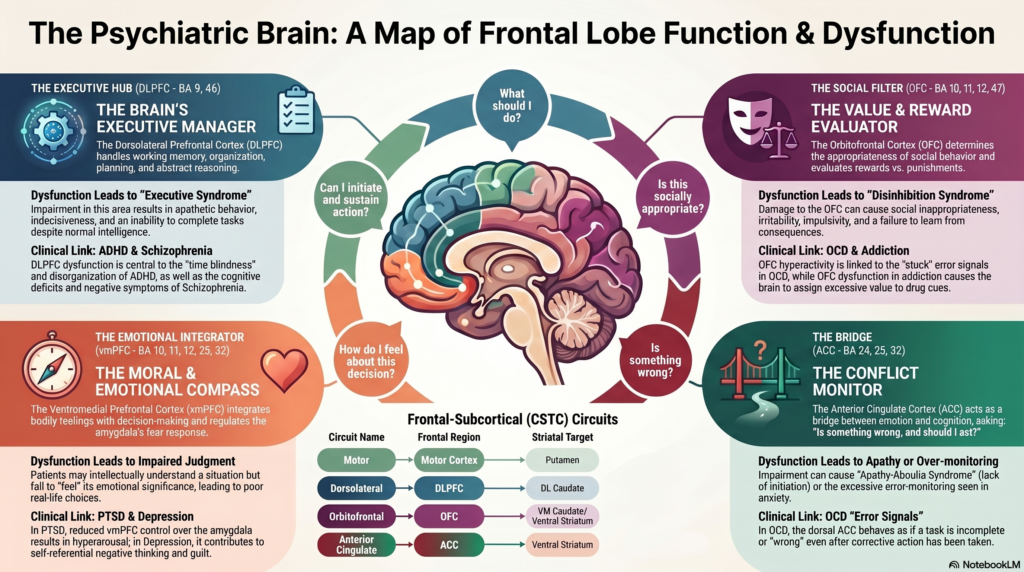
DLPFC — BA 9, 46
The DLPFC is the executive manager of the brain.
Main functions
- Working memory
- Planning
- Organization
- Cognitive flexibility
- Abstract reasoning
- Set shifting
- Problem-solving
- Goal maintenance
- Attention control
- Monitoring of performance
- Suppression of irrelevant information
Clinical syndrome of DLPFC dysfunction
A patient may appear apathetic, poorly organized, distractible, slow, indecisive, and unable to complete tasks despite intact basic intelligence.
Psychiatric relevance
ADHD
DLPFC dysfunction is central to poor working memory, disorganization, time blindness, task initiation problems, and inconsistent performance.
Schizophrenia
DLPFC dysfunction contributes to cognitive deficits, poor working memory, executive dysfunction, negative symptoms, and impaired reality testing.
Depression
Reduced cognitive control from DLPFC may contribute to rumination, poor concentration, indecisiveness, and impaired top-down regulation of limbic distress.
Bipolar disorder
During mania, impaired prefrontal regulation contributes to impulsivity, distractibility, overconfidence, poor judgment, and goal-directed overactivity.
Addiction
DLPFC dysfunction weakens long-term planning and inhibitory control, allowing immediate reward systems to dominate.
3.2 Orbitofrontal Cortex
OFC — BA 10, 11, 12, 47
The OFC is the brain’s value, reward, punishment, and social appropriateness evaluator.
Main functions
- Reward evaluation
- Punishment sensitivity
- Social judgment
- Emotional decision-making
- Reversal learning
- Impulse control
- Updating behaviour when consequences change
- “Is this appropriate?” filtering
The OFC is strongly connected to the amygdala, ventral striatum, hypothalamus, and limbic reward circuits. Orbitofrontal corticostriatal loops are implicated across several psychiatric disorders, including depression, OCD, addiction, and impulsive disorders.
Clinical syndrome of OFC dysfunction
OFC damage produces disinhibition.
The patient may become:
- Impulsive
- Socially inappropriate
- Sexually disinhibited
- Irritable
- Emotionally labile
- Poor at learning from consequences
- Risk-taking
- Lacking tact
- Prone to addictive or compulsive behaviours
Psychiatric relevance
OCD
OFC hyperactivity and abnormal OFC-striatal loops are strongly linked to obsessions, compulsions, error signals, and inability to disengage from perceived threat.
Addiction
The OFC assigns excessive salience to drug cues and immediate rewards.
Mania
OFC under-regulation contributes to disinhibition, overspending, sexual indiscretion, and risky decisions.
Personality disorders
OFC dysfunction may contribute to poor impulse control, emotional lability, anger outbursts, and impaired social judgment.
Frontotemporal dementia
Orbitofrontal involvement can cause early behavioural changes: disinhibition, tactlessness, hyperorality, compulsive behaviours, and poor insight.
3.3 Ventromedial Prefrontal Cortex
vmPFC — medial BA 10, 11, 12, 25, 32
The vmPFC integrates emotion, bodily feeling, memory, value, and decision-making.
Main functions
- Emotional regulation
- Fear extinction
- Self-referential processing
- Moral judgment
- Empathy
- Valuation of future consequences
- Regulation of amygdala activity
- Autonomic-emotional integration
Clinical syndrome of vmPFC dysfunction
The person may intellectually understand a situation but fail to feel its emotional significance. This leads to poor real-life decision-making despite preserved IQ.
Psychiatric relevance
Depression
vmPFC and subgenual anterior cingulate regions are involved in sadness, self-referential negative thinking, guilt, and persistent mood states.
PTSD
Reduced vmPFC regulation over the amygdala may contribute to exaggerated fear, hyperarousal, and impaired extinction of traumatic memories.
Anxiety disorders
Poor vmPFC-amygdala regulation may produce persistent threat perception.
Suicidality
Impaired valuation, hopelessness, emotional pain, and reduced future-oriented thinking may involve medial prefrontal-limbic dysregulation.
Personality pathology
Abnormal vmPFC function may affect empathy, guilt, shame regulation, attachment-related emotional processing, and interpersonal decision-making.
3.4 Anterior Cingulate Cortex
ACC — BA 24, 25, 32
The ACC is a bridge between emotion and cognition. It asks:
“Is something wrong, and should I act?”
The cingulate cortex lies on the medial surface of the cerebral hemisphere and is widely studied because of its role in emotion, cognition, pain, attention, motivation, and psychiatric pathology.
Functional divisions
Dorsal ACC
More cognitive.
Functions:
- Error detection
- Conflict monitoring
- Effort allocation
- Cognitive control
- Response inhibition
- Performance monitoring
Rostral/ventral ACC
More emotional.
Functions:
- Mood regulation
- Emotional pain
- autonomic arousal
- affective salience
- self-related distress
Clinical syndrome of ACC dysfunction
- Apathy
- Reduced motivation
- Poor initiation
- Emotional blunting
- Error-monitoring abnormalities
- Excessive guilt or threat monitoring
- Difficulty shifting away from distressing thoughts
Psychiatric relevance
OCD
The dorsal ACC is involved in error detection and conflict monitoring. In OCD, the brain may behave as though “something is still wrong,” even after corrective action. OCD is associated with dysfunction in inhibitory control involving dACC and wider CSTC circuitry.
Depression
Subgenual and rostral ACC are involved in mood regulation and treatment response.
ADHD
ACC dysfunction contributes to poor error monitoring, inconsistent performance, and reduced task persistence.
Addiction
ACC dysfunction contributes to craving, impaired conflict monitoring, and relapse risk.
Schizophrenia
ACC dysfunction may contribute to impaired self-monitoring, cognitive control deficits, and negative symptoms.
3.5 Frontopolar Cortex
BA 10
The frontopolar cortex is one of the most evolutionarily advanced areas.
Main functions
- Future planning
- Multitasking
- Prospective memory
- Long-term goal representation
- Metacognition
- Reflection on one’s own thinking
- Managing multiple competing goals
Psychiatric relevance
ADHD
Difficulty holding long-term goals in mind while dealing with immediate tasks.
Depression
Excessive self-reflection may turn into rumination.
OCD
Over-monitoring and doubt may involve frontopolar-prefrontal networks.
Schizophrenia
Metacognitive deficits, poor insight, and impaired abstraction may relate to frontopolar dysfunction.
4. Frontal-Subcortical Circuits
Psychiatric symptoms rarely arise from the frontal lobe alone. They arise from circuits.
The major model is the cortico-striato-thalamo-cortical circuit, also called the CSTC loop.
Basic loop
Frontal cortex → Striatum → Globus pallidus/substantia nigra → Thalamus → Back to frontal cortex
These loops regulate movement, cognition, habit, motivation, reward, and emotion. CSTC pathways are involved in movement execution, habit formation, reward processing, inhibitory control, and several psychiatric disorders.
Five major frontal-subcortical circuits
1. Motor circuit
Motor cortex → Putamen → Thalamus → Motor cortex
Relevant to movement disorders, psychomotor slowing, catatonia, antipsychotic-induced extrapyramidal symptoms.
2. Oculomotor circuit
Frontal eye field → Caudate → Thalamus → Frontal eye field
Relevant to eye movement abnormalities, antisaccade deficits, schizophrenia research.
3. Dorsolateral prefrontal circuit
DLPFC → Dorsolateral caudate → Thalamus → DLPFC
Relevant to executive dysfunction, ADHD, schizophrenia, depression, dementia.
4. Orbitofrontal circuit
OFC → Ventromedial caudate/ventral striatum → Thalamus → OFC
Relevant to disinhibition, OCD, addiction, impulsivity, mania, behavioural variant frontotemporal dementia.
5. Anterior cingulate circuit
ACC → Ventral striatum → Thalamus → ACC
Relevant to motivation, apathy, depression, addiction, OCD, suicidality, negative symptoms.
5. Neurotransmitters in Frontal Lobe Function
Dopamine
Essential for working memory, motivation, salience, and executive control.
Too little dopamine in prefrontal cortex may cause:
- Poor attention
- Poor working memory
- Apathy
- Cognitive slowing
- Negative symptoms
Too much or poorly regulated dopamine may contribute to:
- Salience misattribution
- Psychosis
- Impulsivity
- Mania
Noradrenaline
Improves alertness, signal-to-noise ratio, attention, and task persistence.
Relevant to:
- ADHD
- Anxiety
- Stress response
- Arousal regulation
- Executive function under pressure
Serotonin
Regulates mood, impulse control, aggression, patience, and emotional flexibility.
Relevant to:
- Depression
- OCD
- Anxiety
- Impulsivity
- Suicidality
Glutamate
Main excitatory neurotransmitter. Important for learning, plasticity, cognition, and cortical communication.
Relevant to:
- Schizophrenia
- Depression
- OCD
- Ketamine response
- Neurodevelopmental disorders
GABA
Main inhibitory neurotransmitter. Maintains balance, prevents overexcitation, regulates anxiety and cortical rhythm.
Relevant to:
- Anxiety
- Insomnia
- Catatonia
- Seizure-related psychiatric symptoms
- Alcohol and benzodiazepine effects
Acetylcholine
Important for attention, learning, memory, and cognitive flexibility.
Relevant to:
- Dementia
- Delirium
- Attention
- Anticholinergic cognitive burden
6. Frontal Lobe Syndromes
6.1 Dorsolateral Syndrome
“Executive dysfunction syndrome”
Features
- Poor planning
- Poor organization
- Difficulty shifting set
- Working memory deficits
- Concrete thinking
- Poor abstraction
- Reduced verbal fluency
- Distractibility
- Difficulty completing tasks
Common psychiatric overlaps
- ADHD
- Schizophrenia
- Depression
- Bipolar disorder
- Dementia
- Traumatic brain injury
6.2 Orbitofrontal Syndrome
“Disinhibition syndrome”
Features
- Impulsivity
- Irritability
- Poor social judgment
- Inappropriate jokes or comments
- Risk-taking
- Hypersexuality
- Emotional lability
- Poor consequence learning
- Substance misuse
- Compulsive reward-seeking
Common psychiatric overlaps
- Mania
- Addiction
- Personality disorders
- OCD spectrum
- Behavioural variant frontotemporal dementia
- Traumatic brain injury
6.3 Medial Frontal / Anterior Cingulate Syndrome
“Apathy-aboulia syndrome”
Features
- Apathy
- Reduced initiation
- Reduced speech
- Emotional flattening
- Lack of spontaneous activity
- Poor motivation
- Severe cases: akinetic mutism
Common psychiatric overlaps
- Depression
- Negative symptoms of schizophrenia
- Frontal dementia
- Catatonia
- Parkinsonian syndromes
- Post-stroke apathy
7. Role of Frontal Lobe in Major Psychiatric Disorders
7.1 Depression
Depression is not only a “low serotonin” state. It involves disturbed regulation between frontal cognitive-control systems and limbic emotional systems.
Frontal mechanisms
- Reduced DLPFC control → poor concentration, indecision, rumination
- Increased subgenual/medial prefrontal involvement → sadness, guilt, self-referential negative thinking
- ACC dysfunction → impaired motivation, error monitoring, treatment response patterns
- OFC dysfunction → altered reward valuation and anhedonia
Clinical expression
- “I cannot think clearly.”
- “I keep replaying the same thoughts.”
- “I know what to do, but I cannot start.”
- “Nothing feels rewarding.”
7.2 Bipolar Disorder
Mania can be understood as a failure of frontal brakes over limbic-reward systems.
Frontal mechanisms
- Reduced OFC inhibition → disinhibition
- Reduced DLPFC control → distractibility and poor planning
- Abnormal reward circuitry → excessive goal-directed activity
- Impaired vmPFC judgment → underestimation of risk
Clinical expression
- Overspending
- Sexual indiscretion
- Grandiose plans
- Reduced need for sleep
- Rapid decisions without consequence evaluation
7.3 Schizophrenia
Schizophrenia involves distributed brain network dysfunction, but frontal systems are central to cognition, negative symptoms, and self-monitoring.
Frontal mechanisms
- DLPFC dysfunction → working memory deficits
- ACC dysfunction → impaired conflict monitoring and self-monitoring
- Medial prefrontal dysfunction → impaired self-referential processing
- Fronto-temporal dysconnectivity → thought disorder and hallucinations
- Prefrontal dopamine dysregulation → cognitive and negative symptoms
Clinical expression
- Poor planning
- Poor insight
- Thought disorganization
- Reduced motivation
- Cognitive impairment
- Difficulty distinguishing internally generated from externally generated experiences
7.4 OCD
OCD is one of the clearest examples of CSTC circuit dysfunction.
Frontal mechanisms
- OFC overactivity → threat/value overestimation
- ACC overactivity → persistent error signal
- Striatal dysfunction → repetitive habit loops
- Poor inhibitory control → inability to stop compulsions
Clinical expression
The patient does not simply “worry too much.” The brain behaves as if a task remains incomplete.
Examples:
- “Maybe my hands are still contaminated.”
- “Maybe I did not lock the door.”
- “Maybe I harmed someone unknowingly.”
- “It does not feel right yet.”
7.5 ADHD
ADHD is a disorder of regulation, not merely attention.
Frontal mechanisms
- DLPFC dysfunction → working memory and planning problems
- ACC dysfunction → inconsistent effort and error monitoring
- OFC/reward circuitry dysfunction → delay aversion and impulsive reward-seeking
- Frontostriatal dysregulation → poor inhibition and task persistence
Clinical expression
- Knows what to do but does not do it consistently
- Starts many tasks, finishes few
- Works only under pressure
- Poor time estimation
- Emotional impulsivity
- Difficulty delaying gratification
7.6 Addiction
Addiction can be described as reward circuitry overpowering frontal control.
Frontal mechanisms
- OFC assigns excessive value to substance cues
- DLPFC fails to maintain long-term goals
- ACC detects conflict but cannot sustain control
- Ventral striatum drives craving and habit formation
Clinical expression
- “I know it is harmful, but I still do it.”
- Cue-triggered craving
- Relapse despite insight
- Short-term relief overriding long-term goals
7.7 Personality Disorders
Frontal-limbic dysfunction is relevant to impulse control, affect regulation, empathy, and interpersonal judgment.
Possible frontal contributions
Borderline personality patterns
- Reduced emotional regulation
- Impulsivity
- Threat sensitivity
- Poor distress tolerance
Antisocial traits
- Poor fear conditioning
- Reduced punishment sensitivity
- Reduced empathy-related valuation
- Poor moral-emotional integration
Narcissistic traits
- Self-referential processing abnormalities
- Reward and status valuation issues
- Fragile self-regulation
These are not “lesions” in the simple neurological sense, but patterns of network-level regulation shaped by temperament, development, trauma, attachment, and social learning.
7.8 Dementia and Neurocognitive Disorders
Frontal systems are particularly important in behavioural variant frontotemporal dementia.
Features of frontal dementia
- Disinhibition
- Apathy
- Loss of empathy
- Compulsions
- Hyperorality
- Poor judgment
- Socially inappropriate behaviour
- Reduced insight
Differentiation from depression
Depression may present with low motivation, but the patient is often distressed by the change. In frontal dementia, the patient may show poor insight and relatives notice the change more than the patient.
7.9 PTSD and Anxiety Disorders
The frontal lobe regulates threat circuits.
Mechanism
- Amygdala detects threat
- vmPFC helps inhibit fear when safe
- ACC monitors conflict and danger
- DLPFC helps reappraise the situation
In PTSD and anxiety, frontal regulation may be insufficient, leading to persistent threat perception, hypervigilance, avoidance, and intrusive memories.
7.10 Catatonia
Catatonia involves motor, affective, and frontal-subcortical dysregulation.
Possible frontal relevance
- Supplementary motor area dysfunction
- Medial frontal initiation failure
- GABA-glutamate imbalance
- Basal ganglia-thalamocortical dysregulation
This explains why catatonia is not merely “psychological refusal.” It is a brain-state disorder affecting volition, movement, speech, and responsiveness.
8. Frontal Lobe and Core Psychiatric Symptoms
Impulsivity
Often linked to OFC, vmPFC, ACC, and frontostriatal dysfunction.
Seen in:
- ADHD
- Mania
- Substance use disorders
- Personality disorders
- Frontal dementia
Apathy
Often linked to medial frontal and ACC dysfunction.
Seen in:
- Depression
- Schizophrenia
- Parkinson’s disease
- Dementia
- Frontal lesions
Rumination
Linked to medial prefrontal and default mode network overactivity with insufficient DLPFC control.
Seen in:
- Depression
- Anxiety
- OCD
- Trauma-related disorders
Poor insight
Linked to medial and lateral prefrontal dysfunction.
Seen in:
- Psychosis
- Mania
- Dementia
- Addiction
Emotional dysregulation
Linked to impaired frontal regulation of limbic systems.
Seen in:
- ADHD
- Borderline personality disorder
- PTSD
- Bipolar disorder
- Substance use disorders
Executive dysfunction
Linked mainly to DLPFC and frontostriatal circuits.
Seen in:
- ADHD
- Schizophrenia
- Depression
- OCD
- Dementia
- Brain injury
9. Bedside and Clinical Assessment of Frontal Lobe Functions
A. History clues
Ask about:
- Planning
- Time management
- Impulsivity
- Social appropriateness
- Motivation
- Emotional regulation
- Decision-making
- Financial judgment
- Sexual disinhibition
- Addictions
- Repetitive behaviours
- Personality change
Collateral history is often essential because frontal patients may lack insight.
B. Bedside tests
DLPFC tests
- Serial 7s
- Digit span backward
- Verbal fluency: animals, words beginning with F/A/S
- Trail Making Test B
- Similarities and abstraction
- Clock drawing
- Wisconsin Card Sorting Test
OFC tests
- Go/no-go task
- Luria three-step test
- Social judgment questions
- Behavioural observation
- Iowa Gambling Task
ACC/medial frontal tests
- Initiation tasks
- Verbal fluency
- Observation of spontaneous speech and activity
- Apathy scales
- Error-monitoring tasks
10. Frontal Lobe in Psychotherapy
Psychotherapy can be understood partly as strengthening frontal regulation.
CBT
Improves DLPFC-mediated reappraisal, planning, and cognitive control.
DBT
Strengthens frontal inhibition over impulsive limbic reactions.
Exposure and response prevention
Helps recalibrate OFC-ACC threat/error loops in OCD.
Mentalization-based therapy
Enhances medial prefrontal capacity to reflect on self and others.
Schema therapy
Works on frontal-limbic integration of emotional memory, self-concept, and behaviour.
Mindfulness
Improves attentional control, emotional regulation, and meta-awareness.
11. Frontal Lobe and Neuromodulation
Frontal targets are central to modern biological psychiatry.
Left DLPFC
Common target in depression treatment using rTMS.
Rationale: enhance cognitive control and reduce depressive network dominance.
Right DLPFC
Studied in anxiety, inhibitory control, and some depression protocols.
Supplementary motor area
Studied in OCD, tic disorders, and motor inhibition disorders.
Medial prefrontal / ACC regions
Relevant to depression, OCD, addiction, and emotional regulation, though deeper targets are harder to reach non-invasively.
12. Simplified Clinical Map
| Region | Main Function | Dysfunction Looks Like | Disorders |
|---|---|---|---|
| DLPFC | Executive control | Disorganization, poor planning | ADHD, schizophrenia, depression |
| OFC | Social judgment, reward, inhibition | Disinhibition, impulsivity | Mania, addiction, OCD, FTD |
| vmPFC | Emotion-value integration | Poor emotional judgment | Depression, PTSD, personality pathology |
| ACC | Error detection, motivation | Apathy or overchecking | OCD, depression, ADHD |
| SMA | Initiation of action | Akinesia, reduced speech | Catatonia, apathy |
| Broca’s area | Speech production | Non-fluent speech | Aphasia, thought/language disorders |
| Frontal eye field | Voluntary gaze | Eye movement deficits | Schizophrenia research, neurological lesions |
Summary
The frontal lobe is the brain’s regulatory, supervisory, and social-control system.
When it under-functions, patients become impulsive, disorganized, apathetic, emotionally dysregulated, or poorly insightful.
When specific frontal circuits become overactive or stuck, patients may become ruminative, obsessional, hypervigilant, or unable to disengage from threat and error signals.
The frontal lobe answers five core questions:
- What should I do? — DLPFC
- Is this socially appropriate? — OFC
- How do I feel about this decision? — vmPFC
- Is something wrong? — ACC
- Can I initiate and sustain action? — Medial frontal/SMA
In psychiatry, many disorders are disorders of these answers becoming distorted, weakened, exaggerated, or poorly coordinated.
Related posts:
- When the Brain’s CEO Retires Early: Frontal Lobe Syndromes Explained
- How fNIRS Unravels the Mysteries of the Frontal Lobe: A New Window Into the Brain’s Control Center
- Neuropsychiatric Manifestations of Temporal Lobe Epilepsy and Their Clinical Management
- The Origins and Current Relevance of Hypnosis in Psychotherapy
- The Future of Psychodynamic Therapy: Innovations and Enduring Relevance
- Reich and Works : Relevance in Contemporary Therapy