Dysfunctional Beliefs in OCD: Understanding the Mind Behind the Compulsion—and How Therapy Targets It
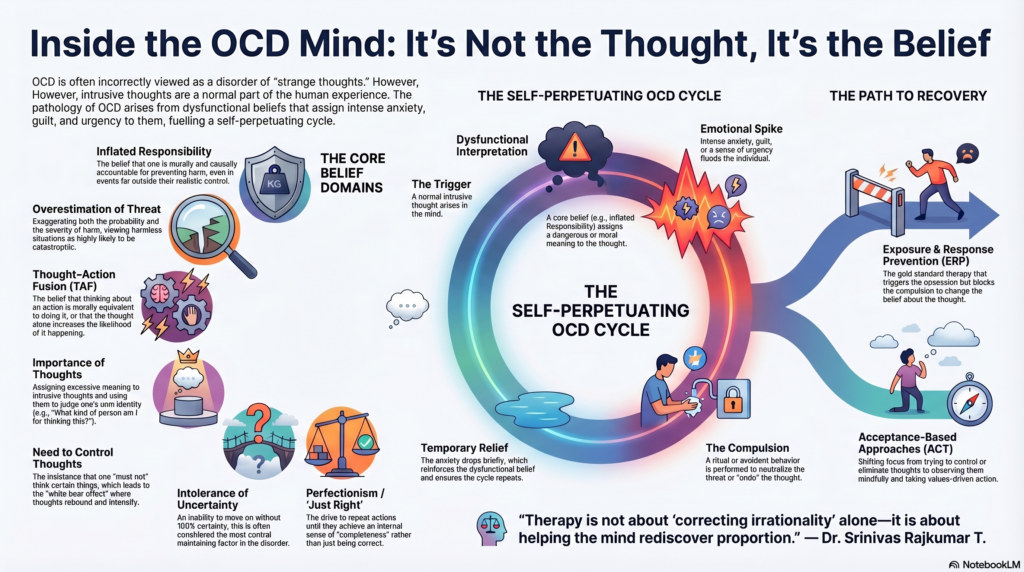 Obsessive-Compulsive Disorder (OCD) is often misunderstood as a disorder of “strange thoughts” or “irrational rituals.” But at its core, OCD is not merely about what a person thinks—it is about what they believe about their thoughts.
Obsessive-Compulsive Disorder (OCD) is often misunderstood as a disorder of “strange thoughts” or “irrational rituals.” But at its core, OCD is not merely about what a person thinks—it is about what they believe about their thoughts.
Most people experience intrusive thoughts:
- “What if I crash the car?”
- “What if I shout something inappropriate?”
- “What if I harm someone?”
These are normal cognitive intrusions.
What differentiates OCD is the interpretation of these thoughts—driven by a set of dysfunctional beliefs that transform harmless intrusions into sources of intense anxiety, guilt, and urgency.
Understanding these beliefs is not just academic—it is central to effective treatment.
The Cognitive Architecture of OCD
The landmark work of the Obsessive Compulsive Cognitions Working Group identified several core belief domains that underpin OCD.
Let us explore these not just as abstract constructs—but as lived psychological realities.
1. Inflated Responsibility
“If something goes wrong, it will be my fault.”
This belief extends personal responsibility far beyond realistic limits. The individual feels morally and causally accountable for preventing harm—even events outside their control.
Clinical manifestation:
- Repeated checking (gas, locks, switches)
- Excessive reassurance seeking
- Avoidance of responsibility-bearing situations
Therapeutic approach:
- Responsibility pie technique: Redistributing responsibility realistically
- Behavioral experiments: Testing what happens when responsibility is not over-assumed
- ERP: Leaving tasks “incomplete” (e.g., checking once and walking away)
2. Overestimation of Threat
“This is highly likely and would be catastrophic.”
Here, both probability and severity of harm are exaggerated.
Clinical manifestation:
- Contamination fears
- Health anxiety within OCD
- Avoidance of perceived “danger zones”
Therapeutic approach:
- Probability re-estimation
- Exposure to feared stimuli without neutralization
- Learning that anxiety ≠ danger
3. Thought–Action Fusion (TAF)
“Thinking it is as bad as doing it—or may make it happen.”
Two forms:
- Moral TAF: Thought = moral wrongdoing
- Likelihood TAF: Thought increases probability
Clinical manifestation:
- Distress about violent/sexual/religious thoughts
- Mental rituals to “undo” thoughts
Therapeutic approach:
- Cognitive distancing: Thoughts are mental events, not actions
- Deliberate exposure to intrusive thoughts (e.g., scripting)
- Reducing neutralization rituals
4. Importance of Thoughts
“This thought must mean something.”
The person assigns excessive meaning to intrusive thoughts.
Clinical manifestation:
- Rumination
- Identity-related distress (“What kind of person am I?”)
Therapeutic approach:
- Normalization of intrusions
- Psychoeducation: “Everyone has these thoughts”
- Defusion techniques (from ACT)
5. Need to Control Thoughts
“I must not think this.”
This leads to paradoxical amplification (the classic “white bear” effect).
Clinical manifestation:
- Thought suppression attempts
- Rebound increase in intrusive thoughts
Therapeutic approach:
- Acceptance-based strategies
- Allowing thoughts without resistance
- Mindfulness: observing thoughts without engagement
6. Intolerance of Uncertainty
“I need 100% certainty.”
Perhaps the most central maintaining factor in OCD.
Clinical manifestation:
- Rechecking
- Reassurance seeking
- Inability to “move on”
Therapeutic approach:
- Uncertainty exposure
- Practicing “maybe, maybe not”
- Building tolerance rather than eliminating doubt
7. Perfectionism / “Just Right” Experiences
“It must feel exactly right.”
Not about correctness—but about internal completeness.
Clinical manifestation:
- Repeating actions until they “feel right”
- Symmetry, ordering compulsions
Therapeutic approach:
- Stopping at ‘imperfect’ states
- Learning that discomfort can be tolerated
- Breaking the link between feeling and action
Additional Clinically Crucial Beliefs
These often operate alongside the core domains:
Magical Thinking
“My actions or thoughts can influence unrelated events.”
Therapy: Behavioral disconfirmation through ERP
Emotional Reasoning
“If I feel anxious, it must be dangerous.”
Therapy: Decoupling emotion from evidence
Memory Distrust
“I cannot trust my memory.”
Therapy: Reducing checking, building tolerance for doubt
Guilt Sensitivity
“I cannot tolerate being responsible for harm.”
Therapy: Exposure to guilt without neutralization
The OCD Cycle (Why These Beliefs Persist)
- Intrusive thought arises
- Dysfunctional belief assigns meaning
- Anxiety / guilt increases
- Compulsion performed (checking, avoidance, mental ritual)
- Temporary relief
- Belief is reinforced
This creates a self-perpetuating loop.
How Therapy Actually Works
1. Exposure and Response Prevention (ERP)
The gold standard.
- Exposure → triggers obsession
- Response prevention → blocks compulsion
What changes?
- Not the thought—but the belief about the thought
2. Cognitive Therapy
Targets the belief layer directly:
- “Is this thought really dangerous?”
- “What evidence supports this belief?”
- “What happens if you do not act on it?”
3. Acceptance-Based Approaches (ACT)
Shift from control to acceptance:
- Thoughts are allowed, not fought
- Focus shifts to values-driven action
The Deeper Shift
Effective therapy does not eliminate intrusive thoughts.
It helps the patient arrive at a fundamentally different stance:
- “This is just a thought.”
- “Uncertainty is okay.”
- “I am not responsible for everything.”
- “I do not need to act on this.”
A Clinical Reflection
In many ways, OCD is a disorder of conscience, responsibility, and control gone into overdrive.
These patients are not careless—they are often hyper-ethical, hyper-aware, and hyper-responsible.
Therapy, therefore, is not about “correcting irrationality” alone—it is about helping the mind rediscover proportion.
Final Word
If we focus only on the ritual, we miss the disorder.
If we understand the belief, we understand the patient.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist
📍 Consultations at: Apollo Clinic Velachery (Opp. Phoenix Mall)
📞 +91-8595155808
✉ srinivasaiims@gmail.com