Stepwise Treatment of Bipolar Depression Based on STEP-BD: What the Landmark Study Teaches Us
 Bipolar depression is one of the most difficult phases of bipolar disorder to treat. Mania is often more visible, disruptive and dramatic, but depression usually causes more long-term suffering, disability, suicide risk, family burden and functional decline.
Bipolar depression is one of the most difficult phases of bipolar disorder to treat. Mania is often more visible, disruptive and dramatic, but depression usually causes more long-term suffering, disability, suicide risk, family burden and functional decline.
The STEP-BD study — Systematic Treatment Enhancement Program for Bipolar Disorder — remains one of the most important real-world studies in bipolar disorder. It was designed to answer practical questions faced by psychiatrists in everyday outpatient care: What helps bipolar depression? Do antidepressants really add benefit? What is the role of psychotherapy? What happens after recovery? Why do patients relapse despite treatment?
STEP-BD was a large NIMH-sponsored, 22-site research collaboration conducted between 1999 and 2005. It enrolled a large, representative group of people with bipolar I and bipolar II disorder, followed them longitudinally, and conducted focused randomized trials relevant to real-world management.
The key message from STEP-BD is clear:
Bipolar depression needs structured, stepwise, long-term care — not casual antidepressant use.
Why STEP-BD matters
Before STEP-BD, many clinicians used antidepressants for bipolar depression, usually along with mood stabilisers. The common assumption was that if a patient was depressed, an antidepressant should help.
STEP-BD challenged this assumption.
It showed that bipolar depression is not simply “depression in a person who also has mania.” It is a different therapeutic problem. The brain is vulnerable not only to depression, but also to switching, mixed states, rapid cycling, residual hypomanic symptoms and relapse.
The study also showed something very important: focused psychotherapy helped recovery more clearly than adjunctive antidepressants in the acute bipolar depression trials.
This is clinically powerful because many patients and families expect bipolar depression treatment to be only medication-based. STEP-BD reminds us that medication is important, but psychotherapy, rhythm regulation, family work and relapse prevention are not optional extras.
STEP-BD lesson 1: Antidepressants are not automatically useful in bipolar depression
The largest STEP-BD bipolar depression trial tested adjunctive antidepressants. Patients with bipolar depression who were already receiving mood stabilisers were randomized to receive either antidepressants — paroxetine or bupropion — or placebo.
The result was striking.
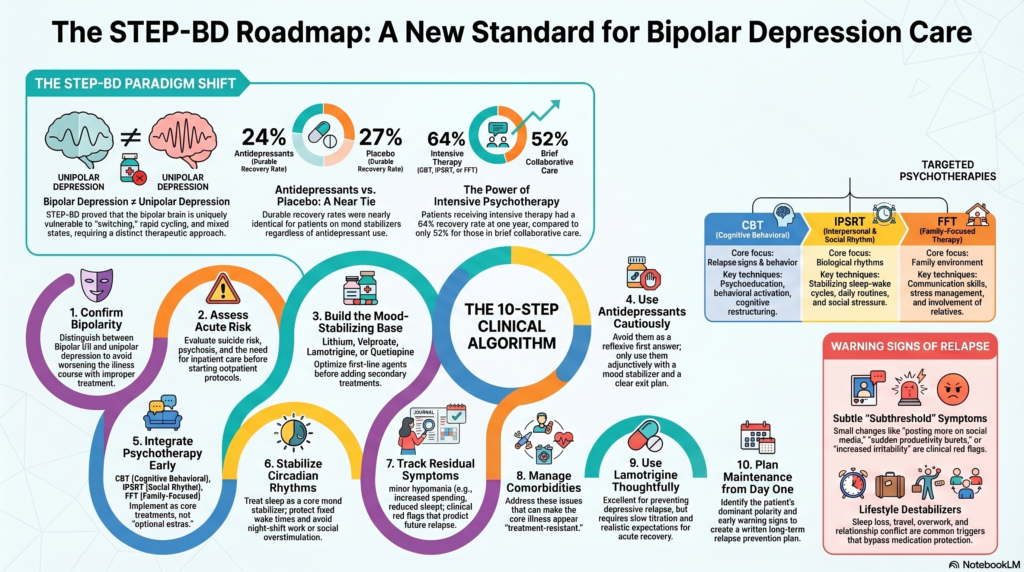
Adjunctive antidepressants did not produce significantly better outcomes than placebo. Durable recovery rates were low in both groups: about 24% with antidepressants and 27% with placebo. Treatment-emergent affective switch rates were also relatively low and similar in both groups, around 10–11%.
This does not mean antidepressants should never be used in bipolar disorder. But it does mean they should not be the reflexive first answer.
The practical lesson is:
Do not treat bipolar depression as unipolar depression.
In bipolar depression, the psychiatrist must first ask:
Is the patient on an adequate mood stabiliser?
Is there mixed activation?
Is sleep reduced?
Is there irritability, agitation or racing thoughts?
Is there past antidepressant-induced switching?
Is there rapid cycling?
Is there substance use?
Is the patient truly depressed, or in a mixed state?
Is there bipolar II depression where cautious antidepressant use may sometimes be considered?
Is psychotherapy available?
Antidepressants may still have a place in selected patients, but usually not as monotherapy, and not as the foundation of long-term bipolar care.
STEP-BD lesson 2: Mood stabilisation is the foundation
In bipolar depression, treatment begins with mood stabilisation.
This includes medicines such as:
lithium,
valproate,
lamotrigine,
quetiapine,
lurasidone,
olanzapine-fluoxetine combination,
cariprazine where available,
and other antipsychotic or mood-stabilising options depending on clinical profile.
STEP-BD was conducted during a period when some newer bipolar-depression-specific options were still emerging. But even then, the study reinforced the principle that bipolar depression should be treated on a mood-stabilising platform.
In practice, before adding an antidepressant, the psychiatrist should ask:
Is lithium at a therapeutic level?
Is valproate adequate?
Is lamotrigine titrated properly?
Is quetiapine or lurasidone indicated?
Is there insomnia requiring a sedating mood-stabilising option?
Is there suicidality where lithium or ECT must be considered?
Is there psychosis requiring antipsychotic treatment?
Is there rapid cycling where antidepressants may be risky?
The first step is not “add antidepressant.”
The first step is stabilise the bipolar illness.
STEP-BD lesson 3: Psychotherapy improves recovery
One of the most useful findings from STEP-BD was the psychotherapy trial.
Patients with bipolar depression receiving pharmacotherapy were randomized to either intensive psychotherapy or a brief collaborative-care psychoeducation intervention.
The intensive psychotherapies included:
Cognitive Behavioural Therapy — CBT
This focused on psychoeducation, relapse warning signs, behavioural activation, problem-solving and cognitive restructuring.
Interpersonal and Social Rhythm Therapy — IPSRT
This focused on stabilising sleep-wake schedules, daily routines, social rhythm regularity and interpersonal stress.
Family-Focused Therapy — FFT
This involved family members and focused on psychoeducation, early warning signs, relapse prevention, stress management and communication.
The results favoured intensive psychotherapy. Patients receiving intensive psychotherapy had higher recovery rates at one year — 64% versus 52% — and recovered faster. Median time to recovery was 169 days with intensive psychotherapy versus 279 days with collaborative care.
This is one of the most important clinical messages from STEP-BD:
In bipolar depression, psychotherapy is not merely supportive counselling. It can accelerate recovery.
Why psychotherapy matters so much in bipolar disorder
Bipolar disorder is highly sensitive to rhythm, stress, sleep disruption, family emotion, interpersonal conflict and medication adherence.
A patient may relapse after:
sleep loss,
night shifts,
travel,
relationship conflict,
substance use,
missed medicines,
irregular routine,
overwork,
festival/social overstimulation,
or stopping medication after feeling better.
Medicines reduce biological vulnerability. Psychotherapy helps the patient manage the lifestyle, behavioural and interpersonal triggers that keep destabilising the illness.
This is why a STEP-BD-informed treatment plan should always include:
psychoeducation,
mood charting,
sleep regularity,
family involvement,
relapse-sign detection,
communication skills,
behavioural activation,
and structured follow-up.
STEP-BD lesson 4: Lamotrigine may help refractory bipolar depression, but expectations must be realistic
STEP-BD also studied refractory bipolar depression — patients who had not responded to antidepressant trials along with mood stabilisers.
A small randomized trial compared add-on lamotrigine, risperidone and inositol. Lamotrigine showed better end-point depression scores and better global functioning than the other options, but recovery rates remained modest. Recovery was around 24% with lamotrigine, 17% with inositol, and 5% with risperidone.
The lesson is balanced.
Lamotrigine can be valuable, especially in bipolar depression and depressive relapse prevention. But it is not a dramatic rescue medicine for acute severe depression. It requires slow titration because of rash risk, and its effects may emerge gradually.
A practical use of lamotrigine:
bipolar II depression,
recurrent depressive polarity,
maintenance after bipolar depression,
patients with poor tolerance to sedating/metabolic medicines,
patients where prevention of depressive relapse is a major goal.
It is less useful when the patient needs rapid anti-manic control, immediate sedation, or urgent treatment for psychotic or suicidal depression.
STEP-BD lesson 5: Recovery is difficult — and relapse is common
STEP-BD’s longitudinal data were sobering.
Among patients who recovered and had follow-up, recurrence was common despite ongoing specialist treatment. Risk of depressive recurrence was linked to factors such as rapid cycling, anxiety disorder, eating disorder history, number of depressive episodes, residual depressive symptoms and residual manic symptoms. Risk of manic/hypomanic/mixed recurrence was associated with rapid cycling, bipolar I subtype, substance abuse, prior manic episodes and residual manic symptoms.
The most clinically important point was this:
Residual subthreshold mood elevation predicted future relapse.
This means that even minor hypomanic symptoms matter.
A patient may say:
“I am only sleeping less.”
“I am just more energetic.”
“I am only slightly irritable.”
“I am just more confident.”
“I am only posting more.”
“I am only spending a little more.”
But these may be early warning signs of relapse.
The STEP-BD message is that bipolar disorder should not be treated only when full episodes occur. The psychiatrist must track and treat residual symptoms.
A STEP-BD-based stepwise algorithm for bipolar depression
Step 1: Confirm bipolar depression, not unipolar depression
Before treatment, the psychiatrist must confirm:
bipolar I or bipolar II disorder,
current depressive episode,
past mania or hypomania,
mixed features,
psychosis,
suicide risk,
substance use,
comorbid anxiety or ADHD,
and previous antidepressant response or switch.
This step is crucial because bipolar depression treated as unipolar depression can worsen the illness course.
Step 2: Assess risk and decide treatment setting
Bipolar depression can be dangerous.
The psychiatrist assesses:
suicidal ideation,
self-harm risk,
psychotic symptoms,
refusal of food,
severe insomnia,
agitation,
mixed features,
substance use,
family support,
and ability to adhere to medication.
Inpatient care or intensive supervision may be needed if risk is high.
Step 3: Build or optimise the mood-stabilising base
The first pharmacological step is to ensure the patient is adequately mood stabilised.
This may involve:
lithium optimisation,
valproate optimisation,
lamotrigine initiation or titration,
quetiapine,
lurasidone,
olanzapine-fluoxetine combination where appropriate,
or other guideline-based bipolar-depression treatments.
The choice depends on the patient’s symptom profile.
For severe suicidality: lithium and/or ECT should be considered.
For insomnia and anxiety: quetiapine may be useful.
For depressive polarity: lamotrigine may be useful.
For psychosis: antipsychotic treatment is required.
For metabolic risk: avoid unnecessarily weight-promoting options where possible.
For women of reproductive age: valproate needs special caution.
Step 4: Do not use antidepressants casually
STEP-BD showed that adjunctive paroxetine or bupropion did not outperform placebo when added to mood stabilisers in bipolar depression.
Therefore, antidepressants should be considered only after careful review.
They may be considered when:
there is clear bipolar depression without mixed features,
the patient is protected by a mood stabiliser,
there is no rapid cycling,
there is no history of antidepressant-induced switch,
the patient has previously responded well,
and close monitoring is possible.
They should be avoided or used very cautiously when:
bipolar I disorder is unstable,
mixed features are present,
sleep is reduced,
there is agitation or irritability,
rapid cycling exists,
substance use is active,
or past antidepressant switching occurred.
The STEP-BD-informed rule:
If you use antidepressants in bipolar disorder, use them cautiously, adjunctively, and with a clear exit plan.
Step 5: Add structured psychotherapy early
STEP-BD strongly supports adding focused psychotherapy to pharmacotherapy.
A psychiatrist should not wait until multiple medications fail before recommending psychotherapy.
The useful psychotherapy targets are:
illness education,
early warning signs,
sleep regularity,
behavioural activation,
family communication,
relapse prevention,
problem-solving,
routine stabilisation,
medication adherence,
and interpersonal stress.
Based on STEP-BD, the major options are:
CBT,
IPSRT,
FFT.
In real-world Indian practice, even if full manualised therapy is unavailable, the psychiatrist can still incorporate the core principles:
track mood and sleep,
protect circadian rhythm,
involve family,
identify relapse signs,
reduce high-emotion conflict,
and create a written relapse plan.
Step 6: Treat sleep as a core mood stabiliser
Sleep is not a side issue in bipolar disorder.
A patient with bipolar depression and poor sleep may slide into mixed agitation or hypomania. A patient recovering from depression may relapse if they resume late nights, night shifts, alcohol use or irregular routines.
A STEP-BD-informed plan should include:
fixed wake time,
regular sleep window,
avoiding all-night work,
reducing late-night phone use,
avoiding alcohol,
monitoring reduced need for sleep,
and family alertness to sleep changes.
IPSRT’s inclusion in STEP-BD highlights how central rhythm stabilisation is in bipolar recovery.
Step 7: Track residual symptoms aggressively
STEP-BD showed that residual symptoms are not harmless. Minor manic symptoms predicted recurrence.
The psychiatrist should regularly ask about:
sleep reduction,
irritability,
increased talking,
racing thoughts,
increased spending,
sexual impulsivity,
increased religious or political intensity,
overconfidence,
increased social media use,
risk-taking,
and sudden productivity bursts.
Depressive residual symptoms should also be tracked:
fatigue,
low interest,
guilt,
poor concentration,
sleep disturbance,
suicidal thoughts,
withdrawal,
and poor functioning.
The goal is not only to treat episodes. The goal is to prevent the next episode.
Step 8: Manage comorbidities
STEP-BD found that recurrence risk was influenced by factors such as anxiety disorders, substance abuse, eating disorder history and rapid cycling.
In clinical practice, this means bipolar depression care must also assess and treat:
alcohol use,
cannabis use,
anxiety disorders,
OCD,
ADHD,
eating disorders,
personality vulnerabilities,
sleep disorders,
thyroid disease,
metabolic syndrome,
and medication non-adherence.
Comorbidities can make bipolar disorder look “treatment-resistant” when the core issue is actually untreated complexity.
Step 9: Use lamotrigine thoughtfully in depressive polarity
STEP-BD’s refractory depression trial supports lamotrigine as a reasonable option, though not a guaranteed solution.
It is especially useful when:
depressive episodes dominate,
maintenance prevention is needed,
sedation must be avoided,
weight gain is a concern,
bipolar II depression is prominent.
However, it must be titrated slowly. Patients must be educated about rash and adherence. Restarting after missed doses may require retitration.
Step 10: Plan maintenance from the beginning
One major mistake is treating bipolar depression as an isolated episode.
The psychiatrist should plan maintenance early:
How many past episodes?
What is the dominant polarity — depression or mania?
Is there rapid cycling?
Is there suicidality?
What medicine prevented relapse before?
What side effects threaten adherence?
What family support exists?
What are the patient’s early warning signs?
What is the plan if sleep reduces?
What is the plan if depression returns?
Maintenance treatment may include lithium, lamotrigine, valproate, quetiapine, antipsychotic maintenance, or combinations depending on illness course.
What STEP-BD changed in the psychiatrist’s thinking
Before STEP-BD, the treatment question was often:
“Which antidepressant should I add?”
After STEP-BD, the better question is:
“Is this patient adequately mood stabilised, rhythm stabilised, psychologically supported and relapse-monitored?”
This is a major shift.
The psychiatrist’s role becomes broader:
diagnose bipolarity accurately,
avoid antidepressant overuse,
optimise mood stabilisers,
use bipolar-specific agents,
add structured psychotherapy,
involve family,
protect sleep rhythm,
monitor residual symptoms,
treat comorbidities,
and prevent relapse.
Practical OPD model based on STEP-BD
First visit
Confirm bipolar diagnosis.
Assess current depression severity.
Ask about mania, hypomania and mixed symptoms.
Assess suicide risk.
Review past medicines.
Review sleep, substances and family support.
Start mood charting.
Begin psychoeducation.
Early follow-up
Optimise mood stabiliser.
Treat sleep.
Avoid antidepressant monotherapy.
Educate family about warning signs.
Monitor for activation.
Add psychotherapy principles.
4–8 weeks
Measure response.
Check adherence and side effects.
If partial response, optimise or augment.
If poor response, re-evaluate diagnosis and comorbidities.
Consider bipolar-depression-specific medicines.
3–6 months
Continue recovery plan.
Treat residual symptoms.
Strengthen routine and family plan.
Monitor work, relationships and functioning.
Review relapse risks.
Long-term
Maintenance treatment.
Mood charting.
Sleep protection.
Substance avoidance.
Early intervention for warning signs.
Regular review of renal, thyroid, liver and metabolic parameters depending on medicine.
Patient-friendly summary
The STEP-BD study teaches that bipolar depression should not be treated like ordinary depression.
Antidepressants such as paroxetine and bupropion did not add clear benefit when used with mood stabilisers in the major STEP-BD trial. Focused psychotherapies such as CBT, IPSRT and family-focused therapy improved recovery rates and helped patients recover faster. Lamotrigine showed some benefit in refractory bipolar depression, but recovery remained difficult. Long-term follow-up showed that relapse is common, especially when residual symptoms, rapid cycling, anxiety, substance use or minor manic symptoms persist.
The best treatment is therefore stepwise:
diagnose correctly,
stabilise mood,
avoid casual antidepressant use,
add structured psychotherapy,
protect sleep and daily rhythm,
treat comorbidities,
track residual symptoms,
involve family,
and plan long-term maintenance.
Conclusion
STEP-BD gave psychiatry a more mature understanding of bipolar depression. It showed that recovery is difficult, antidepressants are not automatically helpful, psychotherapy has real value, lamotrigine may help some refractory patients, and residual symptoms must be taken seriously.
The modern psychiatrist should not chase bipolar depression with repeated antidepressant trials alone. The better approach is structured, biological, psychological and longitudinal.
Mood stabilisation first.
Psychotherapy early.
Antidepressants cautiously.
Sleep rhythm always.
Residual symptoms actively monitored.
Family included.
Relapse prevention built from day one.
That is the STEP-BD-informed way to treat bipolar depression.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808