🌙 Premenstrual Dysphoric Disorder (PMDD): Symptoms, Causes, Diagnosis & Treatment — A Psychiatrist’s Complete Guide
 Premenstrual mood changes are often dismissed as “just PMS.”
Premenstrual mood changes are often dismissed as “just PMS.”
But for a subset of women, the days before menstruation bring intense emotional distress, anger, anxiety, and even suicidal thoughts.
This is not typical PMS.
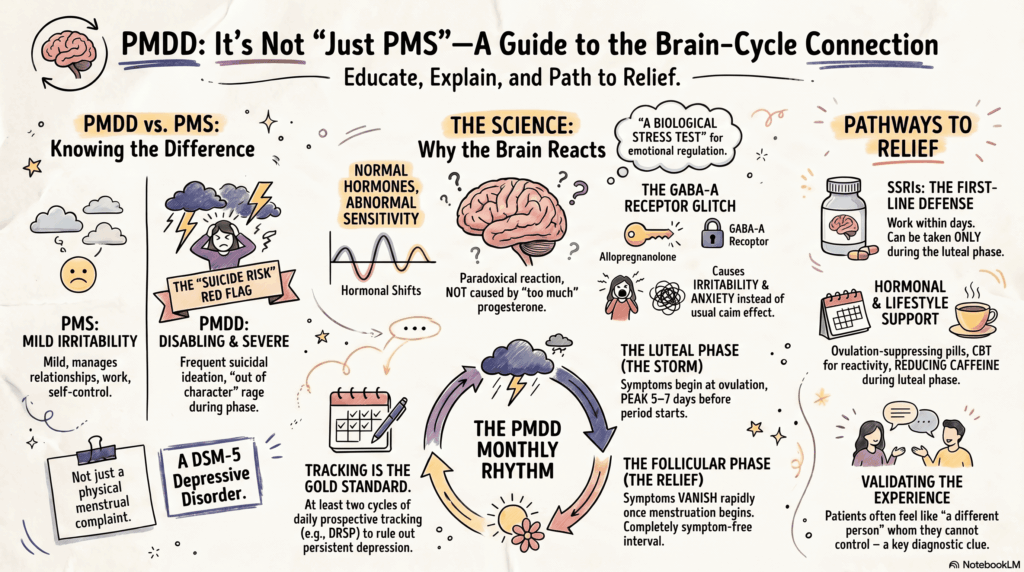
This is Premenstrual Dysphoric Disorder (PMDD)—a serious, underdiagnosed, and highly treatable psychiatric condition.
🔍 What is PMDD? (Understanding Beyond PMS)
PMDD is a cyclical mood disorder linked to the menstrual cycle, classified in DSM-5 under depressive disorders.
Unlike PMS:
- Symptoms are severe and disabling
- There is clear functional impairment
- Symptoms are time-locked to the luteal phase
💡 Key insight: PMDD is not due to abnormal hormone levels—but due to abnormal brain sensitivity to normal hormonal changes.
📊 PMDD vs PMS: The Critical Difference
| Feature | PMS | PMDD |
|---|---|---|
| Severity | Mild–moderate | Severe |
| Functional impairment | Minimal | Significant |
| Mood symptoms | Irritability | Rage, depression, anxiety |
| Suicidal thoughts | Rare | Can occur |
| Diagnosis | Clinical | Requires criteria + tracking |
👉 If relationships, work, or self-control are affected → think PMDD, not PMS
🧠 PMDD Neurobiology: Why the Brain Reacts Differently
PMDD is best understood through the lens of neurosteroid sensitivity.
The key players:
- Progesterone → Allopregnanolone
- Acts on GABA-A receptors
In most individuals:
- GABA modulation → calming effect
In PMDD:
- Paradoxical response
- Leads to:
- Anxiety
- Irritability
- Emotional instability
👉 This explains why:
Symptoms are cyclical but feel psychological, not hormonal
📅 PMDD Symptoms Timeline (The Diagnostic Clue)
PMDD follows a predictable monthly rhythm:
- 🟡 Ovulation → Luteal phase begins
- 🔴 Last 5–7 days before period → Symptoms peak
- 🟢 Within days of menstruation → Rapid relief
- ⚪ Follicular phase → Symptom-free
📌 No symptom-free interval = reconsider diagnosis
⚠️ PMDD Symptoms: What Patients Actually Experience
🔥 Core Emotional Symptoms (Required)
- Severe irritability or anger (“out of character rage”)
- Sudden mood swings or crying spells
- Depressed mood or hopelessness
- Marked anxiety or tension
🧠 Cognitive Symptoms
- Poor concentration
- Feeling overwhelmed
- Negative self-perception
🛌 Physical & Behavioral Symptoms
- Sleep disturbance (insomnia or hypersomnia)
- Fatigue
- Appetite changes/cravings
- Bloating, breast tenderness
🚨 Why PMDD Should Never Be Ignored
PMDD is not just distressing—it can be risky:
- Increased suicidal ideation in luteal phase
- Relationship breakdowns
- Occupational impairment
⚠️ Always assess suicide risk specifically during the symptomatic phase
🔍 How to Diagnose PMDD Correctly
❗ The most common mistake:
Diagnosing based on memory.
✅ The correct method:
📓 Prospective daily symptom tracking (2 cycles minimum)
Tools:
- DRSP (Daily Record of Severity of Problems)
- Symptom diary
👉 This distinguishes PMDD from:
- Major depressive disorder
- Bipolar disorder
- Personality disorders
💊 Best Treatment Options for PMDD
1. SSRIs (First-Line Treatment)
PMDD is unique because SSRIs:
- Work within days (not weeks)
- Can be used in flexible dosing strategies
Options:
- Continuous dosing
- Luteal phase dosing
- Symptom-onset dosing
Common medications:
- Sertraline
- Fluoxetine
- Escitalopram
2. Hormonal Treatments
Goal: Suppress ovulation and hormonal fluctuation
- Combined oral contraceptives
- Drospirenone-containing pills preferred
- GnRH analogues (for severe refractory cases)
3. Psychological & Lifestyle Interventions
- CBT (especially for emotional reactivity)
- Sleep stabilization
- Exercise (modulates stress response)
- Caffeine reduction in luteal phase
4. Nutritional Adjuncts (Supportive Role)
- Calcium supplementation
- Vitamin B6 (limited evidence)
🔄 PMDD Differential Diagnosis (Common Pitfalls)
| Condition | Key Difference |
|---|---|
| Major Depression | Persistent symptoms |
| Bipolar Disorder | Episodic but not cycle-linked |
| Borderline Personality | Emotional instability not phase-specific |
👉 PMDD = Phase-locked symptoms + symptom-free interval
🧭 A Simple Clinical Screening Framework
Ask:
- Do symptoms worsen before periods consistently?
- Is there a clear symptom-free phase?
- Is there functional impairment?
If yes → strongly consider PMDD.
🧠 A Deeper Clinical Perspective
PMDD often coexists with:
- Anxiety traits
- Emotional sensitivity
- Trauma-related vulnerabilities
The menstrual cycle acts as a biological stress test for emotional regulation
🌱 How to Explain PMDD to Patients
Instead of:
❌ “Your hormones are the problem”
Say:
✅ “Your brain is reacting differently to normal hormonal changes”
This reduces:
- Shame
- Self-blame
- Resistance to treatment
💬 Real-Life Impact (What Patients Say)
- “I feel like I become a different person”
- “I know it’s not me, but I can’t control it”
- “Everything feels overwhelming for a few days every month”
👉 These are diagnostic clues—not exaggerations
🧩 Prognosis: The Good News
PMDD is:
- Highly treatable
- Often dramatically responsive to SSRIs
- Manageable with structured care
🌟 Early diagnosis = life-changing improvement
🔚 Final Thought
PMDD sits at a unique intersection of:
- Hormonal physiology
- Brain sensitivity
- Emotional regulation
When recognized:
It transforms from a monthly crisis into a manageable condition.
📍 Need Expert Help for PMDD in Chennai?
If you or your patient experiences severe premenstrual mood changes, a structured psychiatric evaluation can provide clarity and effective treatment.
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
🌐 www.srinivasaiims.com
✉ srinivasaiims@gmail.com 📞 +91-8595155808