Brief Intervention: Making a Difference in a Single Visit for Alcohol Use Disorder
 In an ideal world, every patient struggling with alcohol would have the time, readiness, and resources for long-term treatment. In the real world, clinicians often get one visit—one consultation, one chance to say something that actually sticks.
In an ideal world, every patient struggling with alcohol would have the time, readiness, and resources for long-term treatment. In the real world, clinicians often get one visit—one consultation, one chance to say something that actually sticks.
Brief intervention was designed for exactly this reality.
It accepts a hard truth of clinical practice: change does not always begin with treatment; it often begins with a moment of insight. A single, well-conducted conversation can shift trajectories, soften denial, and open doors that were previously shut.
This is not motivational speaking. It is precision psychiatry applied to time-limited encounters.
Why a Single Visit Still Matters
Alcohol use disorder is typically progressive, but insight fluctuates. Patients often present during windows of ambivalence—after a health scare, family conflict, work problem, or medical investigation. These moments are unstable but powerful.
A brief intervention works because it:
-
Meets the patient where they are, not where we wish they were
-
Respects autonomy rather than provoking resistance
-
Plants a cognitive and emotional marker that continues to work after the visit ends
Even when behaviour does not change immediately, the narrative around alcohol often does. That alone is a therapeutic gain.
The Clinical Sweet Spot for Brief Intervention
Single-visit brief interventions are most effective in:
-
Hazardous or harmful drinking
-
Early or mild alcohol use disorder
-
Patients not actively seeking deaddiction treatment
-
Medical and surgical settings, OPDs, emergency encounters
They are not a substitute for structured treatment in severe dependence—but they often determine whether such treatment is ever accessed.
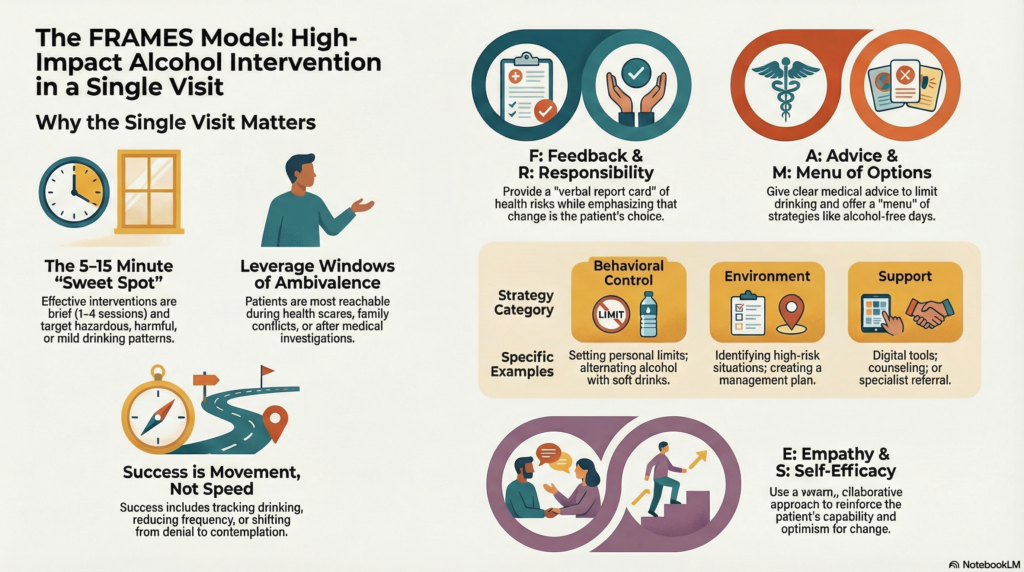
The Core Structure: FRAMES in One Sitting
A single-visit brief intervention works because it is structured, not improvised. The FRAMES model provides this structure.
Feedback: Anchor the Conversation in Reality
Personalized feedback changes the tone instantly. Screening scores (AUDIT/ASSIST), lab abnormalities, sleep disruption, mood symptoms, or blood pressure readings create a shared reference point. The clinician does not accuse; the data speaks.
This shifts alcohol use from a moral issue to a health variable.
Responsibility: Return the Steering Wheel
The most important sentence in a brief intervention is often implicit: “What happens next is your decision.”
When responsibility is acknowledged—not imposed—defensiveness drops.
Paradoxically, autonomy increases engagement.
Advice: Clear, Calm, Medical
Advice is offered once, clearly, and without emotional charge. Reduction or abstinence is framed as a health recommendation, not a demand. The absence of judgement is often what makes the advice memorable.
Menu of Options: Reduce the All-or-Nothing Trap
Many patients reject help because they assume the only option is “total abstinence forever.” A menu reframes change as negotiable and graded:
-
Cutting down
-
Alcohol-free days
-
Avoiding high-risk contexts
-
Counselling or digital tools
-
Medication support
-
Specialist referral
Choice keeps the door open.
Empathy: Normalize the Struggle Without Normalizing the Harm
Empathy acknowledges stress, culture, and habit—without colluding with the behaviour. Avoiding labels matters. Once someone feels understood, they are far more likely to reflect honestly.
Self-Efficacy: Leave the Patient Stronger Than You Found Them
A brief intervention should always end by reinforcing capability. Even a small success—past reduction, brief abstinence, insight itself—is highlighted. Confidence often precedes consistency.
What Success Looks Like After One Visit
A successful brief intervention does not require immediate abstinence.
Success may look like:
-
The patient agreeing to track drinking
-
A reduction in quantity or frequency
-
Acceptance of follow-up or referral
-
A shift from denial to contemplation
-
A remembered sentence that resurfaces weeks later
In alcohol use disorder, movement matters more than speed.
Why This Works: The Science Beneath the Simplicity
Brief interventions work because they intervene before habits fully bypass executive control. At this stage, reflective awareness still engages the prefrontal cortex, especially when feedback is emotionally relevant and non-threatening.
They also avoid a common clinical pitfall: arguing with ambivalence. Ambivalence is not resistance—it is the psychological raw material of change.
The Ethical Power of Brief Intervention
There is something deeply respectful about a single-visit brief intervention. It does not coerce, dramatize, or moralize. It treats the patient as an adult capable of choice, even when those choices are imperfect.
In a busy clinic, this may be one of the highest-impact interventions per minute that a clinician can deliver.
Final Clinical Reflection
Brief interventions remind us that psychiatry is not only about long treatments and complex formulations. Sometimes, it is about saying the right thing, in the right way, at the right moment.
A single visit may not cure alcohol use disorder—but it can change the direction of travel. And in medicine, direction is often destiny.
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
Related posts:
- Why Does Man Need Sex Therapy? A Brief History of Sex Therapy and Human Complexity
- Autism Spectrum Disorder: Early Signs and Intervention
- Autism Spectrum Disorder (ASD) and Ketamine: Emerging Insights from Neurobiology to Potential Intervention
- Artificial Alcohol: Acamprosate – The Sober Solution for Alcohol Dependence
- Summary of The Seven Principles for Making Marriage Work by John Gottman
- The Borderline Mother and the Making of the Borderline Self: Insights from James F. Masterson