The Psychiatric Diagnostic Interview: Where Symptoms, Personality and the Human Story Meet
 A psychiatric consultation is not merely a conversation, a counselling session or an exchange that ends with a prescription. It is a clinical diagnostic procedure in which the psychiatrist listens to the patient’s account, reconstructs the course of illness, observes mental functioning, evaluates risk and develops an initial formulation.
A psychiatric consultation is not merely a conversation, a counselling session or an exchange that ends with a prescription. It is a clinical diagnostic procedure in which the psychiatrist listens to the patient’s account, reconstructs the course of illness, observes mental functioning, evaluates risk and develops an initial formulation.
The patient brings a story. The psychiatrist must understand that story without accepting every first explanation as the final diagnosis.
This requires empathy, but also precision. It requires allowing the patient to speak, but also asking direct questions. It requires understanding distress without automatically validating every interpretation of that distress.
A good psychiatric interview therefore has two simultaneous tasks:
- To understand what the patient is experiencing.
- To determine what those experiences mean clinically.
These are related, but they are not identical.
Psychiatry begins where ordinary conversation ends
Friends, family members and counsellors may listen supportively to a person’s difficulties. The psychiatrist must do something additional: transform a complex account into clinically meaningful patterns.
A complaint such as “I cannot concentrate” may arise from several possibilities:
- Attention-deficit/hyperactivity disorder
- Depression
- Anxiety or obsessive rumination
- Bipolar-spectrum illness
- Sleep deprivation
- Substance use
- Medication effects
- Trauma-related hyperarousal
- Learning disorders
- Neurological or medical illness
- Severe occupational or relationship stress
Similarly, mood swings may represent bipolar disorder, emotional reactivity, trauma, substance-related changes, personality dysfunction, premenstrual symptoms or ordinary responses to rapidly changing circumstances.
Symptoms do not interpret themselves.
The psychiatrist must establish their onset, duration, intensity, context, associated features and consequences before assigning diagnostic significance.
The interview operates on several levels at once
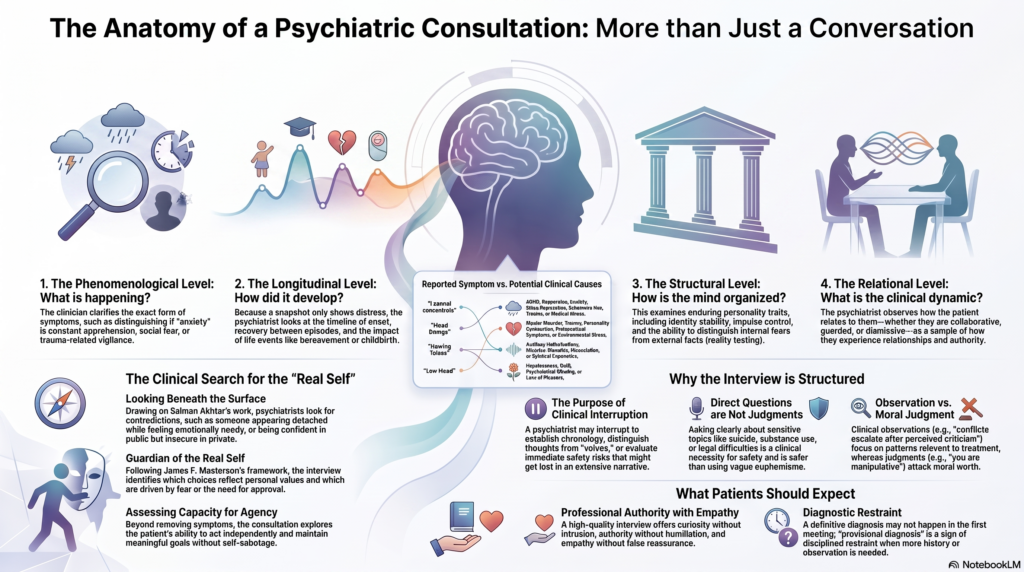
A sophisticated psychiatric interview explores at least four distinct layers.
1. The phenomenological level
This asks: What exactly is happening?
The psychiatrist clarifies the form and content of symptoms:
- Is “anxiety” a constant apprehension, episodic panic, intrusive doubt, trauma-related vigilance or fear of social judgement?
- Is “hearing voices” an auditory hallucination, an intrusive thought, an internal dialogue, dissociation or a culturally understood spiritual experience?
- Is “low mood” accompanied by loss of pleasure, hopelessness, guilt, psychomotor slowing or suicidal thinking?
- Does reduced sleep reflect insomnia with fatigue or a reduced need for sleep with increased energy?
Precise descriptive psychopathology prevents vague words from becoming premature diagnoses.
2. The longitudinal level
This asks: How did the problem develop over time?
Psychiatric diagnosis depends heavily on chronology:
- What came first?
- Was the onset sudden or gradual?
- Were there previous episodes?
- Was there complete recovery between episodes?
- Did symptoms emerge after childbirth, bereavement, sleep deprivation, medication changes or substance use?
- Did attention problems exist in childhood or appear only during adulthood?
- Were there periods of increased energy, reduced sleep, impulsive spending or unusual confidence?
A cross-sectional snapshot may show distress. A longitudinal history reveals the disorder.
3. The structural level
This asks: How is the person’s psychological functioning organised?
Two individuals may report the same symptom while differing greatly in:
- Identity stability
- Emotional regulation
- Impulse control
- Reality testing
- Capacity for intimacy
- Ability to tolerate frustration
- Typical defence mechanisms
- Understanding of self and others
- Moral functioning
- Resilience under stress
Otto Kernberg’s work on structural interviewing shifted attention from merely identifying symptoms to examining the organisation of personality—particularly identity integration, defensive functioning and reality testing. His model helps clinicians distinguish a temporary symptomatic state from a more enduring level of personality organisation.
4. The relational level
This asks: What is happening between the patient and the interviewer?
How a person relates during the consultation may provide important information:
- Does the patient rapidly idealise and then devalue the clinician?
- Is disagreement experienced as abandonment or humiliation?
- Does the person seek reassurance but reject every reassuring explanation?
- Is the interviewer pressured to prescribe, rescue, agree, take sides or assume responsibility?
- Does the narrative remain coherent when difficult questions are asked?
- Can alternative interpretations be considered?
- Is the patient collaborative, guarded, controlling, fearful, seductive, dismissive or unusually compliant?
These observations must never become excuses for labelling or moral judgement. They are hypotheses that require corroboration. Nevertheless, the consultation itself provides a small but valuable sample of how the individual experiences relationships, authority, uncertainty and emotional closeness.
What the patient says—and how it is said
Psychiatric assessment involves more than collecting facts.
The psychiatrist listens to:
- The content of the account
- The sequence of events
- The emotional tone
- Changes in the story
- Contradictions
- Omissions
- The degree of certainty
- The patient’s interpretation of other people’s motives
- The relationship between reported emotion and observed affect
- The capacity to reflect upon one’s own contribution to problems
A person may say, “I am completely calm,” while appearing visibly restless and pressured. Another may deny memory difficulties but repeatedly lose track of the discussion. Someone may describe every previous doctor, employer, friend and partner as incompetent or malicious without considering any alternative explanation.
None of these observations independently establishes a diagnosis. But they contribute to the overall formulation.
Psychiatry examines not only the story but also the psychological processes through which the story is remembered, organised and communicated.
Salman Akhtar: looking beneath the surface
Salman Akhtar’s contribution is particularly relevant because he repeatedly demonstrated that personality cannot be understood from its obvious external presentation alone.
His descriptions often distinguish overt characteristics from less visible covert experiences. A person who appears detached may internally be highly sensitive and emotionally needy. Grandiosity may conceal shame. Excessive independence may conceal an intense fear of dependency. Social confidence may coexist with inner instability.
In his classic work on identity diffusion, Akhtar described features including “contradictory character traits” and “temporal discontinuity.” The first refers to sharply opposing aspects of personality that remain poorly integrated; the second concerns difficulty experiencing one’s life and identity as a coherent continuity across time.
This has an important clinical implication: the psychiatrist must not diagnose only the visible presentation.
The interview explores apparent contradictions:
- Confident in public but profoundly insecure in intimate relationships
- Highly successful professionally but chronically unstable personally
- Desiring closeness while repeatedly withdrawing from it
- Describing oneself as completely independent while being intensely affected by perceived rejection
- Claiming not to care about others’ opinions while organising life around admiration or approval
These contradictions are not necessarily dishonesty. They may reflect compartmentalised states of self, defensive adaptations or poorly integrated identity.
Masterson: searching for the real self
James F. Masterson emphasised the distinction between authentic psychological development and adaptations organised around preserving attachment, approval or emotional survival.
One of the chapter titles in The Search for the Real Self describes the therapist as the “guardian of the real self.”
This phrase captures an important purpose of the diagnostic interview.
The psychiatrist is not simply asking, “What symptoms should be removed?” The deeper questions include:
- What does this person genuinely want?
- Which choices reflect personal values and which are driven by fear?
- Is the person living through an excessively compliant or performative self?
- What happens when they act independently?
- Do autonomy, success or intimacy trigger guilt, emptiness, anxiety or self-sabotage?
- Are symptoms intensified whenever the person attempts to separate from controlling relationships?
Masterson’s framework is especially useful when a person appears outwardly functional but repeatedly abandons meaningful goals, relationships or opportunities whenever emotional independence becomes necessary.
The psychiatric interview therefore investigates not only illness but also the person’s capacity for agency.
Gunderson: making the complex clinically observable
John Gunderson helped transform borderline personality disorder from a vague and often pejorative concept into a more systematically assessable clinical condition.
His diagnostic interview examined five broad areas: “social adaptation, impulse/action patterns, affects, psychosis, and interpersonal relations.”
This is clinically important because personality disorders cannot be diagnosed merely by identifying one dramatic symptom.
Self-harm alone does not establish borderline personality disorder. Neither do anger, unstable relationships, trauma history or emotional sensitivity when considered separately.
The clinician must identify a persistent pattern across several domains:
- Emotional instability
- Relationship patterns
- Identity
- Impulsivity
- Behaviour under stress
- Transient alterations in perception or reality testing
- Occupational and social adaptation
Gunderson’s work also reminds clinicians to assess the patient’s level of functioning rather than focusing exclusively on subjective distress. Two individuals may report equivalent emotional pain but differ substantially in their capacity to work, maintain relationships, control impulses and recover from interpersonal conflict.
Kernberg: symptoms are not the whole personality
Kernberg’s structural approach asks whether a patient has an integrated and reasonably stable understanding of self and others.
For example, can the person recognise that someone they love can also disappoint them without becoming entirely bad? Can they acknowledge both their strengths and limitations without collapsing into worthlessness or grandiosity? Can anger be experienced without destroying the relationship in the mind?
Structural assessment commonly considers:
- Identity integration: Is there a coherent and continuous sense of self?
- Defensive functioning: Does the person predominantly use mature defences, repression, avoidance, splitting, denial or projective processes?
- Reality testing: Can internal fears and interpretations be distinguished from external facts?
- Object relations: Are other people experienced as complex individuals or mainly as idealised, threatening, rejecting or useful figures?
- Aggression and impulse control: How are anger, envy, frustration and destructive impulses managed?
- Moral functioning: Are guilt, responsibility and concern for others integrated or largely driven by fear of punishment and exposure?
This is why some questions in psychiatric interviews may seem more probing than expected. The clinician is not merely compiling symptoms; the clinician is examining how the mind organises experience.
Yalom: the relationship remains essential
A technically accurate diagnosis delivered without human connection may still fail therapeutically.
Irvin Yalom famously wrote:
“It’s the relationship that heals.”
He called this his professional rosary.
This does not mean that the psychiatrist must agree with every belief, avoid difficult questions or provide constant reassurance. It means that clinical truth becomes useful only within a relationship sufficiently safe for the patient to think, reflect and return.
Yalom’s work reminds us that the patient is not merely a collection of symptoms. The interviewer must encounter a person who may be frightened, ashamed, defensive, angry, confused or uncertain about seeking help.
The diagnostic relationship should therefore communicate:
- Curiosity without intrusion
- Authority without humiliation
- Directness without cruelty
- Empathy without false reassurance
- Boundaries without rejection
- Seriousness without emotional coldness
A psychiatrist need not be theatrically cheerful. But clinical seriousness should never become permission for indifference.
Why psychiatrists interrupt
Patients may understandably want to describe their experiences without interruption. The initial narrative is essential, and a good psychiatrist should allow sufficient space for it.
However, psychiatric interviewing cannot remain entirely unstructured.
The clinician may interrupt to:
- Establish chronology
- Clarify what a word means
- Distinguish thoughts from voices
- Separate reduced sleep from reduced need for sleep
- Identify whether a belief is a fear, obsession, overvalued idea or delusion
- Return to an unanswered question
- Evaluate immediate risk
- Prevent important details from being lost in an extensive narrative
An uninterrupted account may be emotionally meaningful but diagnostically incomplete.
The appropriate balance is to begin broadly and progressively narrow the questions. The patient’s spontaneous narrative reveals priorities and subjective meaning; focused questions establish diagnostic reliability.
Interruption becomes problematic when it is dismissive, impatient or prevents essential information from emerging. It is clinically appropriate when it clarifies, organises and protects safety.
Direct questions are not personal accusations
Psychiatrists routinely ask about subjects that are rarely discussed in ordinary conversation:
- Suicidal thoughts
- Self-harm
- Aggression
- Sexual behaviour
- Trauma and abuse
- Substance use
- Medication misuse
- Gambling
- Financial impulsivity
- Domestic violence
- Suspiciousness
- Hallucinations
- Legal difficulties
- Relationship instability
These questions are not evidence that the psychiatrist has already judged the patient.
Direct questioning is often safer than vague euphemism. Asking clearly about suicide does not implant suicidal ideas. Asking about substance use is necessary before prescribing sedatives, stimulants or other psychotropic medication. Asking about sexual behaviour may be important in mania, trauma, compulsive behaviour or medication-related dysfunction.
The clinician should explain why sensitive information is being requested, especially when its relevance may not be obvious.
The difference between observation and judgement
A clinical observation describes a pattern relevant to diagnosis or treatment.
Examples include:
- “There appears to be significant avoidance of situations involving evaluation.”
- “Your concentration difficulties seem to worsen during periods of poor sleep.”
- “Many conflicts appear to escalate after you perceive criticism.”
- “There is a discrepancy between your current account and the previous records.”
- “The requested medication may carry a dependence risk in your situation.”
A judgement attacks the person’s moral worth:
- “You are lazy.”
- “You are impossible.”
- “You are simply manipulative.”
- “Everything is your fault.”
Psychiatry requires the first and should avoid the second.
However, even appropriately phrased clinical observations can feel uncomfortable. A statement does not become judgemental merely because it challenges a preferred explanation. At the same time, clinical accuracy does not excuse unnecessarily harsh delivery.
Both truth and tact matter.
The interview is also a test of diagnostic flexibility
The psychiatrist begins with hypotheses, not conclusions.
During the consultation, the clinician should repeatedly ask:
- What evidence supports the initial diagnosis?
- What evidence contradicts it?
- Could a medical condition explain the presentation?
- Could medication or substance use be contributing?
- Is the reported diagnosis based mainly on an online checklist?
- Are symptoms episodic or longstanding?
- Are there neurodevelopmental factors?
- Is personality influencing the presentation without fully explaining it?
- Is more than one disorder present?
A patient may arrive expecting a particular diagnosis. That expectation deserves respectful consideration, but diagnosis cannot be determined by preference alone.
Similarly, a previous diagnosis should neither be accepted blindly nor rejected merely to appear more insightful. It must be reviewed against the history, mental-status examination, collateral information and longitudinal course.
The mental-status examination: the psychiatric equivalent of physical examination
The mental-status examination is conducted throughout the interview.
The psychiatrist observes:
- Grooming and self-care
- Level of engagement
- Eye contact
- Psychomotor activity
- Speech
- Mood and affect
- Thought organisation
- Thought content
- Perception
- Attention and memory
- Insight
- Judgement
- Impulse control
- Risk
Some findings are directly elicited. Others emerge spontaneously.
Rapid and difficult-to-interrupt speech may support the possibility of an activated mood state. Long response latency may occur in depression, anxiety, cognitive impairment or psychosis. Incongruent affect may require further exploration. Excessive reassurance-seeking may indicate anxiety, obsessive doubt, insecure attachment or another process depending on context.
No single observation is sufficient by itself. Interpretation must remain cautious and culturally informed.
Why diagnosis may remain provisional
Patients sometimes expect a definitive diagnosis during the first meeting. This is possible in some cases but inappropriate in others.
Diagnostic uncertainty may remain when:
- Symptoms have been present only briefly
- The history is incomplete
- Previous records are unavailable
- Substance use complicates the picture
- Mood symptoms overlap with personality patterns
- Childhood information is required
- Family observations differ significantly from the patient’s account
- Cognitive or psychological testing is needed
- Treatment response must be observed over time
A provisional diagnosis is not indecision. It is disciplined restraint.
Psychiatric conditions unfold longitudinally. A responsible psychiatrist may need several consultations before distinguishing bipolar disorder from emotional dysregulation, adult ADHD from anxiety-related inattention, or personality pathology from a temporary crisis.
A diagnostic interview is not psychotherapy—but it can be therapeutic
The primary purpose of the diagnostic interview is assessment. Yet being understood accurately can itself be therapeutic.
A useful formulation may help a patient recognise:
- Why the same relationship pattern keeps recurring
- Why medication alone has not been sufficient
- Why symptoms worsen under particular conditions
- How childhood vulnerabilities interact with present stress
- Why certain coping strategies provide short-term relief but long-term harm
- Which aspects are symptoms and which are enduring patterns
- What can realistically change
Yalom’s emphasis on relationship, Masterson’s protection of the real self, Gunderson’s operational clarity, Akhtar’s attention to hidden contradictions and Kernberg’s structural depth are not competing philosophies. Together, they describe a richer psychiatric assessment.
The patient must be heard as a person, examined as a patient and understood as a mind developing across time.
What patients should reasonably expect
A high-quality psychiatric diagnostic interview should offer:
- Adequate opportunity to describe the main concern
- Focused clarification of symptoms and chronology
- Respectful assessment of sensitive subjects
- Review of medical conditions, medications and substance use
- Mental-status and risk assessment
- An explanation of the likely diagnosis or differential diagnosis
- Discussion of treatment options
- Clarity about uncertainty
- A follow-up plan
- Opportunities to ask relevant questions
Patients should not expect every clinical conclusion to confirm their own initial interpretation. They should expect the reasoning to be explained respectfully.
What psychiatrists owe their patients
Professional authority carries responsibilities.
The psychiatrist should:
- Listen before concluding
- Ask directly without humiliating
- Distinguish observation from moral judgement
- Explain the purpose of sensitive questions
- Avoid premature diagnosis
- Recognise personal countertransference
- Consider cultural and linguistic context
- Admit uncertainty
- Reassess when new evidence emerges
- Maintain confidentiality and boundaries
- Communicate the treatment plan clearly
The psychiatrist’s task is not to be liked at every moment. But neither is it enough merely to be technically correct.
Clinical authority is strongest when it is combined with clarity, restraint and respect.
Conclusion: clarity is part of compassion
The psychiatric diagnostic interview is one of medicine’s most sophisticated clinical instruments. It combines descriptive psychopathology, longitudinal reasoning, observation, risk assessment, personality evaluation and human relationship.
It must be empathic—but not vague.
It must be direct—but not demeaning.
It must be structured—but not mechanical.
It must recognise suffering—but also examine the beliefs, behaviours and relationship patterns that may perpetuate that suffering.
The best psychiatric interview does not merely ask, “What diagnosis does this person have?”
It also asks:
Who is this person? How has their mind adapted? What is hidden beneath the presenting symptom? What happens under stress? What remains healthy? And what form of treatment offers the greatest possibility of meaningful change?
That is the difference between issuing a prescription and practising psychiatry.
About the Author
Dr. Srinivas Rajkumar T
MD Psychiatry, AIIMS New Delhi
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery, Chennai
Opposite Phoenix Marketcity
Email: srinivasaiims@gmail.com
Phone: +91-8595155808