Methylphenidate vs Atomoxetine: Which ADHD Medicine Has a Better Sexual Side-Effect Profile?
 Sexual side effects are among the most under-discussed problems in ADHD treatment. Patients may talk about sleep, appetite, anxiety, focus, or irritability, but they often hesitate to mention changes in libido, erection, ejaculation, orgasm, or sexual confidence.
Sexual side effects are among the most under-discussed problems in ADHD treatment. Patients may talk about sleep, appetite, anxiety, focus, or irritability, but they often hesitate to mention changes in libido, erection, ejaculation, orgasm, or sexual confidence.
This silence matters.
For adults with ADHD, sexual functioning is not a “minor” quality-of-life issue. It affects self-esteem, relationships, intimacy, treatment adherence, and long-term confidence in medication. A patient may stop an otherwise effective medicine simply because no one warned them about a sexual side effect or because they felt too embarrassed to bring it up.
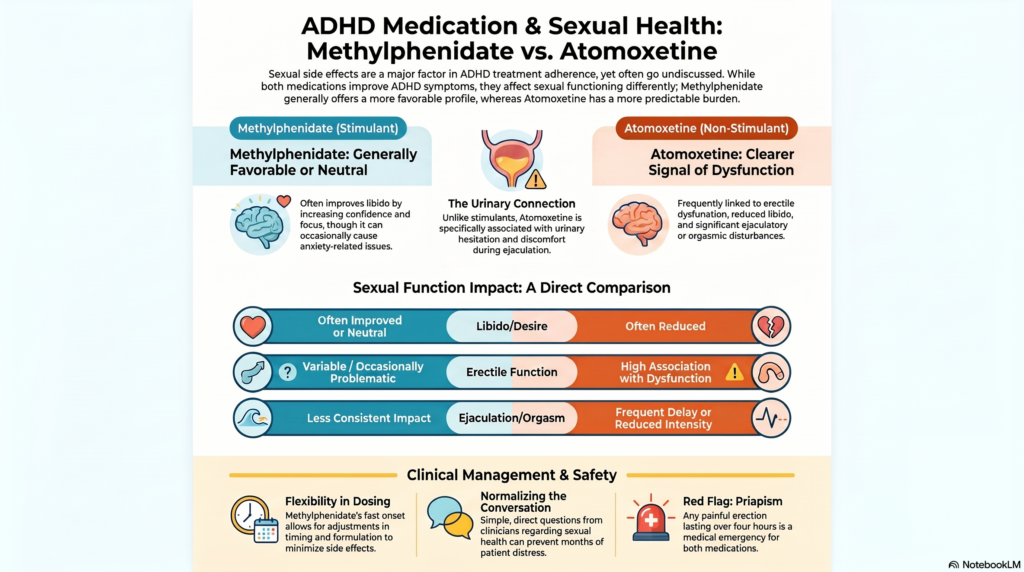
Among the commonly used medications for ADHD, two names often come up: methylphenidate and atomoxetine. Both can be useful. Both can improve ADHD symptoms. But when it comes to sexual side effects, they are not equal.
In clinical practice, methylphenidate usually has a more favourable sexual side-effect profile than atomoxetine.
That does not mean methylphenidate is completely free of sexual adverse effects. It is not. But the pattern, predictability, and burden of sexual side effects are generally more concerning with atomoxetine, especially in adult males.
Why Sexual Side Effects Matter in ADHD Treatment
ADHD is not just about attention. It affects emotional regulation, impulse control, motivation, planning, relationship stability, and self-confidence. These factors can directly influence sexual functioning.
Many adults with ADHD already struggle with:
- Performance anxiety
- Inconsistent desire
- Difficulty staying mentally present during intimacy
- Impulsive sexual behaviour
- Relationship conflict
- Low self-esteem from years of underperformance
- Depression or anxiety as comorbid conditions
- Substance use or pornography-related concerns in some cases
When ADHD medication works well, sexual functioning may actually improve indirectly. A person may feel calmer, more confident, more emotionally regulated, more attentive to their partner, and less overwhelmed. This is one reason why stimulant treatment, including methylphenidate, can sometimes improve sexual confidence rather than worsen it.
But medications can also create new sexual problems. That is why choosing the right medicine matters.
Methylphenidate and Atomoxetine: A Brief Difference
Methylphenidate is a stimulant medication. It mainly improves dopamine and noradrenaline signalling in brain circuits involved in attention, motivation, and executive control. It often works quickly, sometimes from the first dose, though proper dose titration still takes time.
Atomoxetine is a non-stimulant medication. It selectively increases noradrenaline signalling and usually takes longer to show full benefit. It may be useful when stimulants are contraindicated, poorly tolerated, misused, or ineffective.
The difference in mechanism is important because sexual functioning is closely connected to dopamine, noradrenaline, serotonin, anxiety systems, vascular tone, and autonomic nervous system balance.
Dopamine is generally linked to motivation, reward, desire, and sexual drive. Noradrenaline can improve focus and alertness, but excessive noradrenergic tone may also contribute to anxiety, erectile difficulty, delayed ejaculation, urinary hesitation, or a sense of physical tension.
This partly explains why atomoxetine has a more recognisable pattern of sexual and genitourinary side effects.
The Key Clinical Difference
The simplest way to explain the difference is this:
Methylphenidate has a variable sexual profile. Atomoxetine has a more predictable sexual side-effect burden.
With methylphenidate, some patients experience no sexual side effects. Some report improved libido, better confidence, and better sexual engagement because ADHD symptoms are better controlled. A smaller group may experience reduced libido, erectile difficulty, delayed ejaculation, anxiety-related performance issues, or rare prolonged erections.
With atomoxetine, sexual side effects are more clearly recognised, especially in adults. These may include reduced libido, erectile dysfunction, ejaculation delay, ejaculation disorder, orgasmic difficulty, and urinary hesitation.
So, when a patient specifically asks, “Which medicine is less likely to disturb sexual functioning?” the answer is usually:
Methylphenidate is generally the more favourable option, provided it is otherwise clinically appropriate.
Libido: Desire May Improve with Methylphenidate, But Reduce with Atomoxetine
Libido is not just a hormonal phenomenon. It is affected by mood, sleep, stress, relationship quality, confidence, anxiety, and brain reward systems.
In adults with ADHD, low libido may come from multiple causes:
- Depression
- Anxiety
- Chronic stress
- Poor sleep
- Relationship conflict
- Low self-worth
- Pornography or compulsive sexual behaviour patterns
- Substance use
- Previous antidepressant exposure
- Hormonal problems
- Medical illness such as diabetes, obesity, hypertension, or thyroid disease
Methylphenidate may improve libido in some patients by improving drive, motivation, focus, confidence, and emotional regulation. Some patients feel more “present” and less scattered during intimacy. However, if the dose is too high, or if it causes anxiety, palpitations, irritability, insomnia, or appetite suppression, libido may reduce.
Atomoxetine is more likely to be associated with reduced libido. This may be due to noradrenergic effects, emotional blunting in some patients, physical discomfort, urinary symptoms, or delayed orgasm/ejaculation affecting sexual satisfaction.
So, from a libido perspective, methylphenidate is often more favourable.
Erectile Dysfunction: Atomoxetine Has a Clearer Signal
Erectile function depends on vascular health, psychological comfort, autonomic balance, nitric oxide pathways, testosterone, relationship context, and medication effects.
Methylphenidate can occasionally contribute to erectile difficulty, especially if it increases anxiety, sympathetic arousal, restlessness, or vascular constriction. But this is not usually one of its most prominent or predictable adverse effects.
Atomoxetine has a clearer association with erectile dysfunction in adults. In clinical practice, this is one of the more important reasons adult male patients may dislike or discontinue atomoxetine. Some describe it as difficulty getting an erection, difficulty maintaining erection, reduced rigidity, or reduced confidence due to inconsistent performance.
A key point is that erectile dysfunction from medication is often misread as psychological failure. The patient may think, “Something is wrong with me,” when the actual explanation may be pharmacological, dose-related, or interaction-related.
This is why clinicians should ask directly and respectfully.
A simple question like, “Any change in erection, ejaculation, desire, or orgasm after starting the medication?” can prevent months of distress.
Ejaculation and Orgasm: Atomoxetine Is More Likely to Cause Delay or Disturbance
Ejaculatory problems are particularly important with atomoxetine.
Patients may report:
- Delayed ejaculation
- Difficulty ejaculating
- Reduced orgasm intensity
- Ejaculation without normal pleasure
- Ejaculatory discomfort
- Rarely, unusual spontaneous ejaculation-like experiences
These symptoms can be deeply distressing. Patients may not volunteer them unless asked.
Methylphenidate can also affect ejaculation in some individuals, but the pattern is less consistent. Some patients may experience faster ejaculation if anxious, delayed ejaculation if overstimulated or tense, or improved control if ADHD-related impulsivity improves. The effect depends heavily on dose, timing, baseline anxiety, relationship context, and comorbid conditions.
Atomoxetine, in contrast, has a more recognisable noradrenergic sexual side-effect pattern.
So, when ejaculation delay or orgasmic difficulty is a major concern, atomoxetine needs careful counselling.
Urinary Symptoms: The Often-Forgotten Clue
Atomoxetine can cause urinary hesitation or difficulty passing urine in some adults. This matters because sexual and urinary systems are closely linked through autonomic nervous system pathways.
A patient may not initially say, “I have sexual dysfunction.” Instead, he may say:
- “Urine is not flowing freely.”
- “I have to wait before passing urine.”
- “I feel I am not emptying fully.”
- “There is discomfort during ejaculation.”
- “Sex feels different after starting the tablet.”
These complaints should not be ignored.
Urinary hesitation with atomoxetine can coexist with erectile or ejaculatory problems. In men with pre-existing prostate symptoms, anxiety, pelvic floor tension, or autonomic sensitivity, atomoxetine may be less comfortable.
Methylphenidate is not commonly associated with this same pattern of urinary hesitation.
This is another reason methylphenidate often feels cleaner in day-to-day tolerability.
Priapism: Rare but Important With Both
Both methylphenidate and atomoxetine have rare warnings related to priapism.
Priapism means a prolonged, often painful erection that persists beyond sexual stimulation. It is a medical emergency, especially if it lasts more than four hours, because delayed treatment can damage erectile tissue.
With methylphenidate, rare cases have been reported, sometimes after dose increases or during withdrawal/drug holidays. With atomoxetine, priapism has also been reported rarely.
This should be explained without alarming the patient. The message is simple:
If an erection is painful, unusually prolonged, or lasts more than four hours, seek emergency medical care.
This is rare, but it is important enough that every male patient should know it.
Why Methylphenidate Often Has a More Favourable Profile
There are several practical reasons.
1. Faster onset and easier attribution
Methylphenidate acts quickly. If a side effect appears, it is often easier to link it to timing, dose, or formulation. This makes adjustment easier.
Atomoxetine takes longer to work and is taken continuously. Side effects may build gradually, and patients may struggle to identify when the problem began.
2. Flexible dose timing
Methylphenidate can often be adjusted by changing:
- Immediate-release vs extended-release formulation
- Morning dose
- Afternoon booster
- Total daily dose
- Timing in relation to work, sleep, and intimacy
This flexibility can help when side effects are time-linked.
Atomoxetine is less flexible in this sense. It is usually a daily medication with a more continuous pharmacological effect.
3. Less predictable sexual dysfunction signal
Methylphenidate can cause sexual side effects, but many patients experience no sexual dysfunction. Some improve. The overall pattern is more variable and often manageable.
Atomoxetine has a more established adult sexual dysfunction signal, especially for erectile and ejaculatory problems.
4. Better fit for many adults with ADHD
Many adult ADHD guidelines place stimulants, including methylphenidate, as first-line options when medication is indicated. Atomoxetine is often used when stimulants are not suitable, not tolerated, or ineffective.
This does not make atomoxetine a bad medicine. It simply means that for many adults, methylphenidate is considered earlier in the medication pathway.
When Atomoxetine May Still Be the Better Choice
A balanced discussion is important. Atomoxetine is not an inferior medicine for every patient. It may be useful when:
- There is high risk of stimulant misuse
- There is a history of substance use disorder where stimulants are unsuitable
- Stimulants worsen anxiety, insomnia, tics, appetite, or blood pressure
- The patient prefers a non-stimulant option
- There are occupational or regulatory concerns around stimulant use
- Stimulants are contraindicated
- There is poor response to stimulant trials
In some patients, atomoxetine works well and causes no sexual side effects. In others, the sexual side effects are mild or manageable.
The key is not to avoid atomoxetine completely. The key is to counsel properly and monitor actively.
Practical Counselling Before Starting ADHD Medication
Before starting either methylphenidate or atomoxetine, clinicians should normalise the discussion.
A useful explanation is:
“ADHD medicines can sometimes affect sexual desire, erection, ejaculation, orgasm, or urinary flow. These effects are not your fault, and they are usually manageable. Please tell me early if you notice any change.”
This single statement reduces shame.
It also helps differentiate medication side effects from anxiety, depression, relationship problems, or pre-existing sexual dysfunction.
What to Ask During Follow-Up
At follow-up, instead of asking only, “Any side effects?”, it is better to ask specific questions:
- Has your libido changed?
- Any difficulty with erection?
- Any delay or change in ejaculation?
- Any change in orgasm or sexual satisfaction?
- Any urinary hesitation or reduced urine flow?
- Any painful or prolonged erection?
- Did the problem start after the medicine or dose change?
- Does it vary with timing of the dose?
- Is the ADHD benefit worth the side effect, or should we adjust?
Patients often answer more honestly when the clinician asks in a matter-of-fact way.
Managing Sexual Side Effects
Management depends on the drug, symptom, severity, and patient priorities.
Possible strategies include:
- Reducing the dose
- Changing timing
- Changing formulation
- Waiting briefly if side effects are mild and early
- Switching from atomoxetine to methylphenidate if appropriate
- Switching from methylphenidate to another stimulant or non-stimulant if needed
- Reviewing antidepressants, especially SSRIs
- Checking substance use, sleep, anxiety, depression, diabetes, hypertension, and hormonal factors
- Considering drug interactions
- Addressing relationship and performance anxiety
- In selected cases, evaluating erectile dysfunction medically
In atomoxetine-related sexual dysfunction, it is especially important to check for CYP2D6 interactions. Medicines such as fluoxetine, paroxetine, and bupropion can increase atomoxetine exposure and may worsen side effects in some patients.
A Clinical Rule of Thumb
A practical way to summarise the comparison is:
Methylphenidate: usually sexually neutral or sometimes beneficial, but occasionally problematic.
Atomoxetine: useful non-stimulant, but more likely to produce sexual and urinary side effects in adults.
Therefore, when sexual side effects are a major concern, methylphenidate usually has the more favourable profile.
The Bigger Picture: Treat the Person, Not Just the ADHD
Medication choice should never be mechanical. The best ADHD medicine is not simply the one with the strongest symptom score improvement. It is the one the patient can actually live with.
A good treatment plan considers:
- ADHD symptom control
- Sleep
- Appetite
- Anxiety
- Mood stability
- Blood pressure and pulse
- Substance use risk
- Occupational needs
- Relationship functioning
- Sexual health
- Long-term adherence
- Patient preference
Sexual side effects are not cosmetic. They are clinically meaningful.
A patient who feels embarrassed, disconnected, or sexually impaired may quietly stop treatment. A patient who feels understood is more likely to continue treatment safely and honestly.
Final Takeaway
Both methylphenidate and atomoxetine can be effective ADHD medications. But their sexual side-effect profiles differ.
For many adults, methylphenidate has a more favourable sexual side-effect profile. It is often neutral, sometimes beneficial, and usually easier to adjust if problems occur. Atomoxetine remains a valuable non-stimulant option, but it has a clearer association with erectile dysfunction, ejaculatory problems, reduced libido, orgasmic changes, and urinary hesitation.
The most important clinical step is simple: ask about sexual side effects openly, respectfully, and routinely.
When ADHD treatment improves attention but damages intimacy, the treatment plan is incomplete.
When ADHD treatment improves attention, confidence, relationships, and quality of life, it is doing what it is meant to do.
Need Help With Adult ADHD Assessment or Treatment?
Adult ADHD can be easily missed, especially when it presents with anxiety, procrastination, emotional dysregulation, relationship strain, career inconsistency, or long-standing executive dysfunction.
A careful assessment should look beyond a checklist. It should include developmental history, functional impairment, comorbid anxiety or depression, sleep, substance use, personality factors, medical contributors, and treatment goals.
I provide structured assessment and evidence-based treatment planning for adults with ADHD, including medication selection, dose optimisation, side-effect monitoring, and practical strategies for day-to-day functioning.
For consultations and ADHD-related clinical guidance, you can reach out through:
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery, Chennai
Opp. Phoenix Mall
Email: srinivasaiims@gmail.com
Phone: +91-8595155808
The goal is not just to prescribe a tablet. The goal is to help you function better, feel more in control, and build a life that works with your brain rather than against it.