Schizophrenia as a Disorder of Brain Networks: A Reader-Friendly Explanation
 Schizophrenia is often explained through dopamine, hallucinations, delusions, or “chemical imbalance.” While these ideas are important, modern neuroscience is showing us a broader and more nuanced picture: schizophrenia may also be understood as a disorder of brain connectivity.
Schizophrenia is often explained through dopamine, hallucinations, delusions, or “chemical imbalance.” While these ideas are important, modern neuroscience is showing us a broader and more nuanced picture: schizophrenia may also be understood as a disorder of brain connectivity.
In simple terms, schizophrenia is not just about one brain chemical or one brain region going wrong. It may involve difficulties in how different brain networks communicate, coordinate, and regulate one another.
This idea is called the dysconnectivity hypothesis of schizophrenia.
The review paper “Revisiting Functional Dysconnectivity: A Review of Three Model Frameworks in Schizophrenia” brings together recent resting-state fMRI research from 2017–2023 and explains how altered brain connectivity may be linked to symptoms such as hallucinations, delusions, disorganized thinking, poor attention, reduced motivation, motor abnormalities, and executive dysfunction.
What Does “Dysconnectivity” Mean?
The brain does not work like a set of isolated departments. It works more like a highly coordinated city.
There are roads, traffic signals, control centres, emergency systems, and communication hubs. If one road is blocked, traffic may reroute. If signals malfunction, the entire system may become inefficient.
Similarly, the brain depends on smooth communication between networks. In schizophrenia, the problem may not be only that one region is “overactive” or “underactive,” but that the communication between regions becomes poorly regulated.
This is what researchers mean by functional dysconnectivity: abnormal coordination between brain circuits.
Some connections may become too strong. Others may become too weak. The result is not simply “less brain activity,” but a disturbed pattern of communication.
Two Important Network Systems in Schizophrenia
The paper focuses mainly on two major network systems:
- Cerebello-thalamo-cortical circuits
- The Triple Network system
Both are important, but they explain different aspects of schizophrenia.
1. Cerebello-Thalamo-Cortical Circuit: The Brain’s Coordination Loop
The cerebellum is traditionally known for movement and coordination. But modern neuroscience has shown that it also contributes to cognition, timing, prediction, and emotional regulation.
The thalamus acts like a relay station. It filters and routes information to the cortex.
The cortex, especially the prefrontal cortex, is involved in planning, judgment, attention, working memory, and reality testing.
Together, the cerebellum, thalamus, and cortex form a coordination loop.
In schizophrenia, this loop may show both:
- Hyperconnectivity, where some pathways are overconnected
- Hypoconnectivity, where other pathways are underconnected
This uneven connectivity may help explain why some patients have disturbances in movement, thought organisation, and sensory processing.
Why Motor Symptoms Matter in Schizophrenia
Motor symptoms in schizophrenia are often under-recognised. These may include:
- Reduced spontaneous movement
- Abnormal posturing
- Slowness
- Catatonic features
- Subtle coordination difficulties
- Medication-independent motor abnormalities
The reviewed studies suggest that abnormal connectivity between the motor cortex, thalamus, and cerebellum may be associated with these motor features.
This is clinically important because schizophrenia is not only a disorder of hallucinations and delusions. It is also a disorder that affects the body, movement, timing, and behaviour.
The Neurodevelopmental Model
One of the strongest explanations for cerebello-thalamo-cortical dysconnectivity is the neurodevelopmental model.
This model suggests that schizophrenia may emerge from altered brain development, especially during childhood, adolescence, and early adulthood.
The adolescent brain normally undergoes major refinement. Connections are strengthened, weakened, or pruned depending on experience and biological programming. If this developmental process is disturbed, the brain may enter adulthood with poorly tuned communication systems.
This may explain why schizophrenia often begins in late adolescence or early adulthood.
The paper highlights that disrupted thalamo-cortical development may be linked to early psychotic symptoms and increasing symptom severity. In simple language, the “wiring and tuning” of the brain’s major relay systems may be altered before full illness becomes visible.
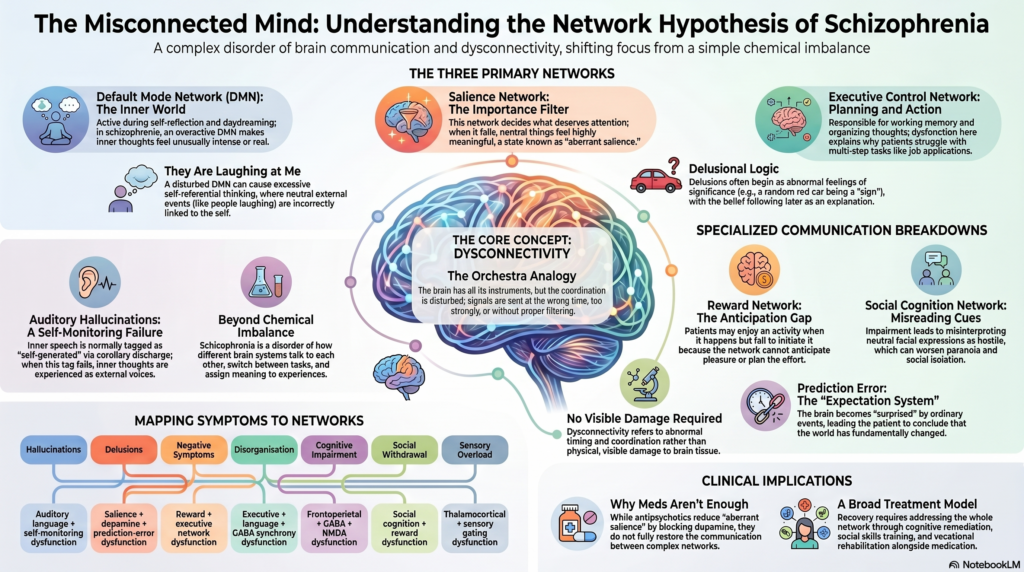
2. The Triple Network: The Brain’s Control, Self, and Salience System
The second major framework discussed in the paper is the Triple Network model.
This includes three large-scale brain networks:
A. Default Mode Network
The Default Mode Network, or DMN, is active when we are internally focused.
It is involved in:
- Self-reflection
- Autobiographical memory
- Inner thoughts
- Imagination
- Theory of mind
- Thinking about oneself and others
In schizophrenia, altered DMN activity may be linked to excessive self-referential thinking, unusual interpretations, or difficulty distinguishing internal thoughts from external reality.
B. Central Executive Network
The Central Executive Network, or CEN, is active when we need to solve problems, focus, plan, and hold information in mind.
It is closely related to:
- Working memory
- Attention
- Planning
- Cognitive flexibility
- Decision-making
- Executive control
In schizophrenia, dysfunction in this network may contribute to poor concentration, difficulty planning, disorganised work habits, and reduced problem-solving ability.
This is especially relevant because cognitive symptoms often predict real-world functioning better than hallucinations or delusions alone.
C. Salience Network
The Salience Network, or SN, helps the brain decide what is important.
It detects emotionally or biologically relevant information and helps switch the brain between internal focus and external task focus.
In simple terms, the salience network asks:
“What should I pay attention to right now?”
In schizophrenia, abnormal salience processing may cause neutral events to feel unusually meaningful. This may contribute to ideas of reference, paranoia, hallucinations, and disorganised attention.
For example, a casual glance from a stranger may feel personally significant. A random sound may feel like a signal. An ordinary event may be interpreted as having hidden meaning.
This is one reason why the salience network is so important in modern explanations of psychosis.
The Salience Network and Psychosis
One of the most clinically useful ideas is that schizophrenia may involve aberrant salience.
Normally, the brain filters thousands of stimuli every second. Most are ignored. Only relevant information becomes conscious and meaningful.
In psychosis, this filtering system may become disturbed.
As a result:
- Irrelevant stimuli may feel important
- Internal thoughts may feel externally generated
- Coincidences may feel intentional
- Background noise may become meaningful
- Ordinary experiences may acquire unusual emotional weight
This can help us understand the lived experience of psychosis in a more compassionate way.
The patient is not “making things up.” Their brain may be assigning abnormal importance to internal or external experiences.
How Triple Network Dysconnectivity Explains Symptoms
Triple network dysfunction may contribute to several symptom domains:
Hallucinations
If sensory information is poorly filtered and salience is wrongly assigned, internally generated experiences may be selected into conscious awareness as if they were real external perceptions.
Delusions
If neutral events feel intensely meaningful, the mind may create explanations for them. Over time, these explanations may become fixed beliefs.
Disorganised thinking
Poor coordination between executive control and salience processing may make it difficult to organise thoughts, shift attention, and maintain logical flow.
Negative symptoms
Reduced motivation, social withdrawal, and emotional flattening may be linked to disrupted reward, dopamine, and executive networks.
Cognitive impairment
Working memory, processing speed, attention, and planning may be affected when executive networks do not communicate efficiently with other systems.
Neurotransmitters Still Matter — But They Are Part of a Larger Network Story
The network model does not reject dopamine, glutamate, serotonin, or GABA theories. Instead, it places them inside a broader systems framework.
Dopamine may influence salience and reward. Glutamate and GABA may affect excitation-inhibition balance. Serotonin may influence mood, perception, and large-scale network activity.
In other words, neurotransmitters are not isolated chemicals floating around randomly. They shape how networks communicate.
This is why schizophrenia cannot be reduced to “too much dopamine” alone. Dopamine matters, but it is part of a larger brain network disturbance.
The Vulnerability-Stress Model
The paper also discusses the vulnerability-stress framework.
This model suggests that schizophrenia may arise when biological vulnerability interacts with environmental stress.
The vulnerability may include:
- Genetic risk
- Neurodevelopmental differences
- Altered dopamine function
- Glutamate or GABA imbalance
- Early brain connectivity changes
Stressors may include:
- Trauma
- Substance use
- Sleep disruption
- Social adversity
- Urban stress
- Migration
- Family conflict
- Academic or occupational pressure
When vulnerability and stress combine, the brain’s regulatory systems may become overwhelmed, increasing the risk of psychotic symptoms.
This model is especially useful clinically because it reminds us that schizophrenia is not purely biological and not purely psychological. It is a disorder at the intersection of brain, development, environment, and lived experience.
A Simple Clinical Translation
We can understand schizophrenia through three interacting layers:
1. Developmental Layer
The brain’s circuits may develop differently from childhood to adolescence.
2. Chemical Layer
Dopamine, glutamate, GABA, and serotonin systems may become dysregulated.
3. Network Layer
Large-scale networks may fail to coordinate smoothly.
When these layers interact, symptoms may emerge.
Positive symptoms such as hallucinations and delusions may reflect abnormal salience, sensory filtering, and dopamine-linked network dysfunction.
Negative symptoms may reflect reduced motivation, reward dysfunction, and poor network integration.
Cognitive symptoms may reflect executive network impairment and disrupted coordination between the prefrontal cortex, thalamus, cerebellum, and salience systems.
Why This Matters for Treatment
This network-based view has important implications.
Schizophrenia treatment should not focus only on reducing hallucinations or delusions. It should also address:
- Cognition
- Motivation
- Sleep
- Stress regulation
- Social functioning
- Family environment
- Substance use
- Physical activity
- Rehabilitation
- Occupational functioning
- Emotional regulation
Medication remains central, especially for acute psychosis and relapse prevention. But recovery is broader than symptom suppression.
A network-informed approach supports combining:
- Antipsychotic medication
- Psychoeducation
- Cognitive remediation
- Family intervention
- Social skills training
- Sleep stabilisation
- Stress reduction
- Substance-use treatment
- Vocational rehabilitation
- Structured routines
- Early intervention services
The future of schizophrenia care will likely move toward more personalised models, where clinical symptoms, cognitive testing, imaging, digital markers, and functional outcomes are integrated.
Schizophrenia Is Not a Single Broken Switch
The most important message from this review is that schizophrenia is unlikely to be explained by one abnormal chemical, one damaged region, or one simple cause.
It is better understood as a disorder of coordination.
The brain’s timing, filtering, prediction, salience, and executive systems may stop working in harmony.
This explains why schizophrenia can affect perception, thought, emotion, motivation, movement, and social functioning at the same time.
It also gives us a more humane way to understand the illness.
The person with schizophrenia is not simply “irrational.” Their brain may be struggling to organise reality because its communication systems are dysregulated.
Conclusion
The dysconnectivity model gives us a powerful framework for understanding schizophrenia.
The cerebello-thalamo-cortical system helps explain motor symptoms, cognitive slowing, and developmental vulnerability.
The triple network model helps explain hallucinations, delusions, attention problems, self-referential thinking, and executive dysfunction.
The neurotransmitter and vulnerability-stress models help explain why these network disturbances emerge and worsen in certain individuals.
Together, these models move us away from simplistic explanations and toward a more integrated view of schizophrenia: a disorder of brain development, chemistry, connectivity, stress response, and meaning-making.
This is the direction modern psychiatry is moving toward — not just controlling symptoms, but understanding the whole brain, the whole person, and the whole life context.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery Opp. Phoenix Mall
✉ srinivasaiims@gmail.com 📞 +91-8595155808