Evidence-Based Therapies in Body Dysmorphic Disorder (BDD)
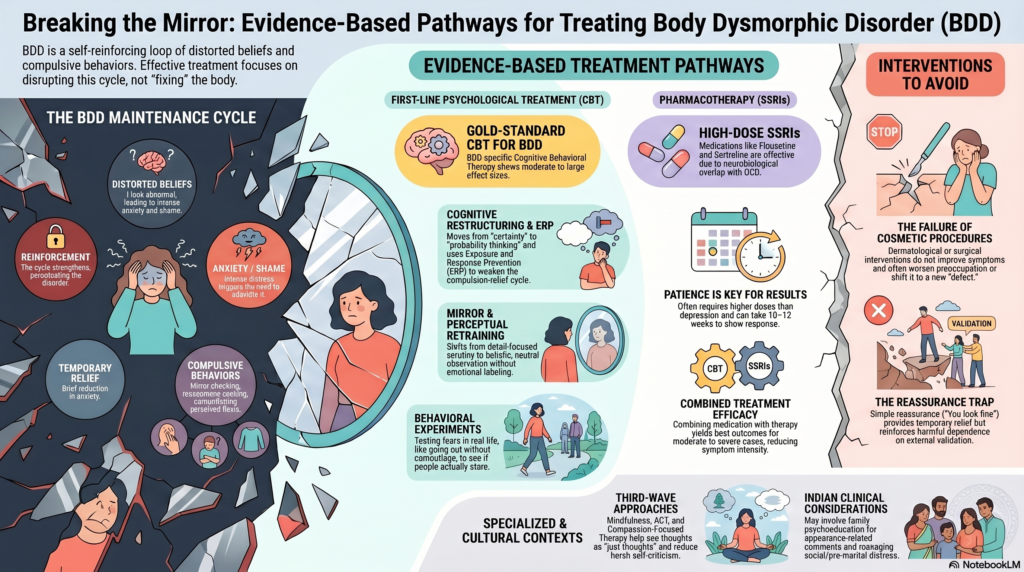 Body Dysmorphic Disorder is characterized by preoccupation with perceived defects in appearance, often accompanied by repetitive behaviours (mirror checking, camouflaging) and poor insight. It lies on the obsessive–compulsive spectrum, and the strongest evidence base reflects this.
Body Dysmorphic Disorder is characterized by preoccupation with perceived defects in appearance, often accompanied by repetitive behaviours (mirror checking, camouflaging) and poor insight. It lies on the obsessive–compulsive spectrum, and the strongest evidence base reflects this.
1. Cognitive Behavioral Therapy (CBT) – First-Line Psychological Treatment
Core Principle
BDD is maintained by a loop of:
- Distorted beliefs → anxiety/shame → compulsive behaviours → temporary relief → reinforcement
Key Components (BDD-specific CBT)
a. Cognitive Restructuring
- Identifies beliefs such as:
- “I look abnormal”
- “Others will reject me”
- Challenges:
- Evidence for/against the belief
- Alternative interpretations
- Moves from certainty → probability thinking
b. Exposure and Response Prevention (ERP)
Adapted from OCD treatment:
- Exposure:
- Looking in mirrors in a structured way
- Going out without camouflage
- Attending social situations
- Response Prevention:
- Avoiding checking, reassurance seeking, or hiding
👉 This directly weakens the compulsion–relief cycle
c. Mirror Retraining
- Shifting from detail-focused scrutiny → holistic, neutral observation
- Avoiding emotional labeling (“ugly”, “bad”)
- Learning to tolerate seeing oneself without reacting
d. Perceptual Retraining
- Addresses visual processing bias (over-focusing on minor flaws)
- Helps patients process faces/bodies more globally rather than selectively
e. Behavioral Experiments
- Testing beliefs in real-life settings
- Example: “If I don’t camouflage, people will stare” → tested in controlled exposure
Evidence
- Multiple RCTs show moderate to large effect sizes
- Considered gold-standard psychotherapy for BDD
2. Pharmacotherapy – SSRIs (Strong Evidence Base)
First-Line Medications
- High-dose SSRIs (e.g., fluoxetine, sertraline, escitalopram)
Why SSRIs?
- BDD shares neurobiological overlap with OCD
- Reduces:
- Obsessive preoccupation
- Compulsive behaviours
- Associated depression/anxiety
Key Clinical Points
- Often require higher doses and longer duration than depression
- Response may take 10–12 weeks
- Effective even in patients with poor insight or delusional intensity
3. Combined Treatment (CBT + SSRI)
- Best outcomes in moderate to severe BDD
- Medication reduces symptom intensity → improves engagement in therapy
- Therapy builds long-term cognitive and behavioral change
4. Metacognitive and Third-Wave Approaches (Emerging Evidence)
a. Mindfulness-Based Interventions
- Reduce over-identification with thoughts:
- “I look ugly” → seen as a thought, not a fact
- Promote body neutrality rather than forced positivity
b. Acceptance and Commitment Therapy (ACT)
- Focus:
- Accepting internal experiences
- Acting according to values rather than appearance concerns
c. Compassion-Focused Therapy (CFT)
- Particularly useful where shame is central
- Develops:
- Self-soothing
- Reduction of harsh self-criticism
5. Interventions with Limited or No Benefit
Cosmetic Procedures
- Dermatological or surgical interventions
❌ Do not improve BDD symptoms
❌ Often worsen preoccupation or shift focus to new “defects”
Reassurance-Based Approaches
- “You look fine”
❌ Temporarily relieving
❌ Reinforces dependence on external validation
6. Managing Severe or Complex Cases
In severe BDD:
- Poor insight / delusional beliefs
- Social isolation
- Suicidality
Management includes:
- Intensive CBT
- High-dose SSRIs
- Close monitoring
- In select refractory cases:
- Antipsychotic augmentation (limited evidence)
7. Indian Clinical Context
In practice, additional therapeutic focus may include:
- Addressing family reinforcement of appearance concerns
- Managing pre-marital or event-triggered exacerbations
- Working with comparison-driven distress (social and familial)
Therapy often includes:
- Psychoeducation for family
- Boundary setting around appearance-related comments
Final Clinical Takeaway
The most effective treatment for BDD involves:
Targeting the cognitive distortions, behavioral compulsions, and emotional processes—not the body itself.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
If you encounter patients with persistent appearance-related distress, early identification and structured, evidence-based intervention can significantly improve outcomes and prevent chronicity.
Related posts:
- Therapy in Body Dysmorphic Disorder (BDD): What Actually Helps
- Body Dysmorphic Disorder (BDD): An Indian Perspective
- How Society Shapes the Presentation of Body Dysmorphic Disorder
- 🧠 Are Antidepressants Meant for Life? How to Stop Safely with a Time-Limited, Evidence-Based Approach
- Evidence-Based tDCS Protocols: A Practical Clinical Guide
- Exposure and Response Prevention (ERP): How Evidence-Based Therapy Breaks the OCD Cycle