Young Mania Rating Scale (YMRS): How to Interpret Severity, Define Remission, and Use It in Real-World Practice
 In clinical psychiatry, diagnosing mania is only the beginning. The real challenge lies in measuring severity, tracking improvement, and deciding when recovery is meaningful—not just numerical. This is where the Young Mania Rating Scale (YMRS) becomes indispensable, particularly in the management of Bipolar Disorder.
In clinical psychiatry, diagnosing mania is only the beginning. The real challenge lies in measuring severity, tracking improvement, and deciding when recovery is meaningful—not just numerical. This is where the Young Mania Rating Scale (YMRS) becomes indispensable, particularly in the management of Bipolar Disorder.
This comprehensive guide integrates original research, practical interpretation, evidence-based thresholds, and copyright clarity—so you can use YMRS with both precision and integrity.
📚 Original Paper
Young RC et al. (1978)
A rating scale for mania: reliability, validity and sensitivity
British Journal of Psychiatry
What the original study established:
- A brief 11-item clinician-rated scale
- High inter-rater reliability (~0.93)
- Strong validity against clinical impressions
- Sensitivity to treatment-related change
👉 Importantly, the original paper did not define rigid severity categories. It provided approximate anchor points based on clinical correlation.
🔹 What Does YMRS Measure?
The YMRS assesses manic symptoms over the past 48 hours, combining:
- Patient report
- Clinician observation
Structure:
- 11 items
- Score range: 0–60
- Weighted scoring (0–4 and 0–8 items)
Core domains:
- Elevated mood
- Motor activity
- Reduced need for sleep
- Irritability
- Pressured speech
- Thought disorder
- Insight and disruptive behavior
🔹 What Did the Original Paper Say About Severity?
The original authors suggested approximate anchors, not strict categories:
- ~13 → Minimal
- ~20 → Mild
- ~26 → Moderate
- ~38 → Severe
👉 These were descriptive correlations, not diagnostic cut-offs.
🔹 Modern Severity Interpretation (Clinically Derived)
Over time, clinicians and researchers developed practical bands for usability:
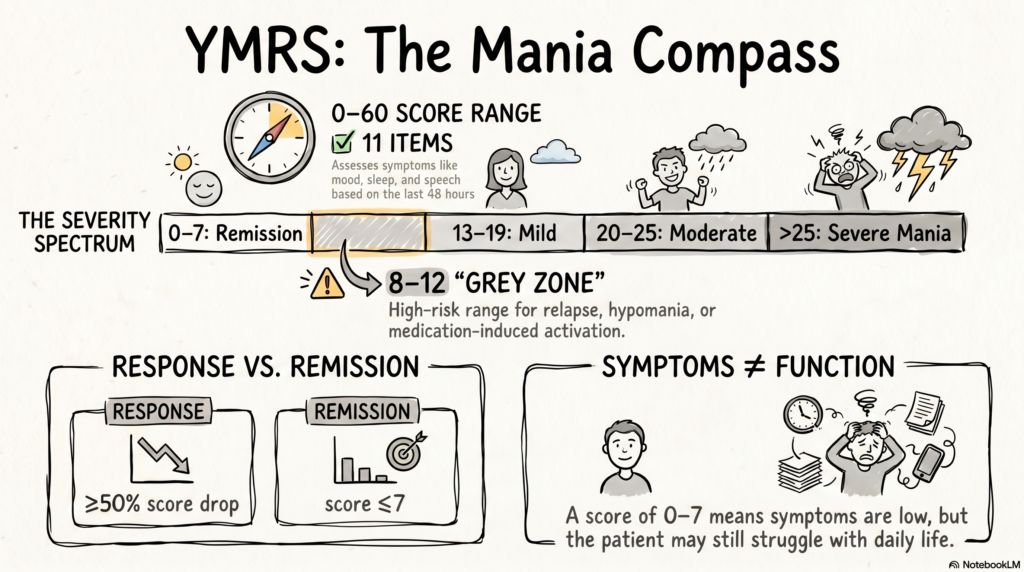
- 🟢 0–7 → Remission / Euthymia
- 🟡 8–12 → Subthreshold Mania
- 🟠 13–19 → Mild Mania
- 🔴 20–25 → Moderate Mania
- 🔴 >25 → Severe Mania
Important:
👉 These are consensus-based, not original paper definitions
🔹 Defining Remission: Evidence-Based Practice
👉 YMRS ≤ 7 = Remission
This threshold is widely used in:
- Clinical trials
- Treatment guidelines
- Longitudinal outcome studies
Supporting evidence:
- Many trials use:
- YMRS ≥20 → Inclusion (acute mania)
- ≤7 or ≤12 → Remission thresholds
- Observational data (e.g., EMBLEM study):
- Scores ~25 correspond to marked illness severity
🔹 Treatment Response vs Remission
YMRS allows dynamic tracking:
- ≥50% reduction → Treatment response
- ≤7 → Remission
Example:
- Baseline: 32
- Follow-up: 14
→ Response achieved, but not remission
👉 This distinction prevents premature tapering or discharge
🔹 The Critical “Grey Zone” (YMRS 8–12)
This range is clinically high-risk and underappreciated.
Patients may be:
- Improving but unstable
- At risk of relapse
- Hypomanic
- Experiencing medication-induced activation
👉 Requires:
- Close follow-up
- Medication optimization
- Psychoeducation
🔹 Symptomatic vs Functional Remission
A key clinical insight:
👉 Symptomatic remission ≠ Functional recovery
A patient with:
- YMRS = 6
- Persistent sleep disturbance, irritability, or impulsivity
→ Not truly recovered
Stricter approach:
👉 YMRS ≤ 5 → Stringent remission
🔹 Evidence Base: Why YMRS Remains the Gold Standard
Across decades, YMRS has shown:
1. Strong Psychometric Properties
- High reliability
- Good internal consistency
- Valid across populations
2. Sensitivity to Change
- Detects improvement within 1–2 weeks of treatment
3. Research Relevance
- Widely used in major studies (e.g., STEP-BD)
- Primary outcome measure in bipolar trials
🔹 Limitations: Where YMRS Needs Clinical Judgment
No scale is sufficient on its own.
Key limitations:
- Measures symptoms, not functioning
- May under-detect irritable/dysphoric mania
- Depends on patient insight and cooperation
👉 Always integrate:
- Clinical interview
- Collateral history
- Functional assessment
🔹 Copyright and Ethical Use
The YMRS originates from a published journal article and is not strictly public domain.
Ownership:
- Associated with British Journal of Psychiatry publication rights
Practical reality:
It is widely treated as a freely usable clinical tool for:
- Routine practice
- Teaching
- Research (with citation)
Use caution when:
- Reproducing full scale in commercial apps
- Publishing in books or proprietary platforms
Best practice:
✔ Credit original authors
✔ Avoid unnecessary verbatim reproduction
✔ Use interpretations and summaries
🔹 Practical OPD Framework
Use YMRS as a clinical compass:
- >25 → Crisis phase (consider admission)
- 20–25 → Active stabilization
- 13–19 → Residual symptoms
- 8–12 → Relapse watch zone
- ≤7 → Remission → Plan maintenance
🔹 A Clinician’s Reflection
“YMRS tells us when mania has reduced.
But recovery is when the patient regains sleep, judgment, and meaningful engagement with life.”
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
If you are seeking structured, evidence-based care for bipolar disorder or mood instability, consultations are available.