ISSTD and the Gold Standard Treatment of Dissociation
 A definitive, clinically grounded overview for modern psychiatric practice
A definitive, clinically grounded overview for modern psychiatric practice
Dissociative disorders have long occupied a complex and often misunderstood space within psychiatry. Oscillating between neurology, psychology, and trauma science, their management has historically been fragmented—at times overly biological, at others overly interpretive. It is within this landscape that the International Society for the Study of Trauma and Dissociation has emerged as a central organizing force.
The ISSTD represents the most authoritative global body dedicated to the understanding and treatment of trauma-related and dissociative disorders. Its clinical guidelines—particularly those addressing dissociative identity disorder (DID)—have shaped what is now widely accepted as the gold standard: the phase-oriented model of treatment.
🔷 Why ISSTD Matters
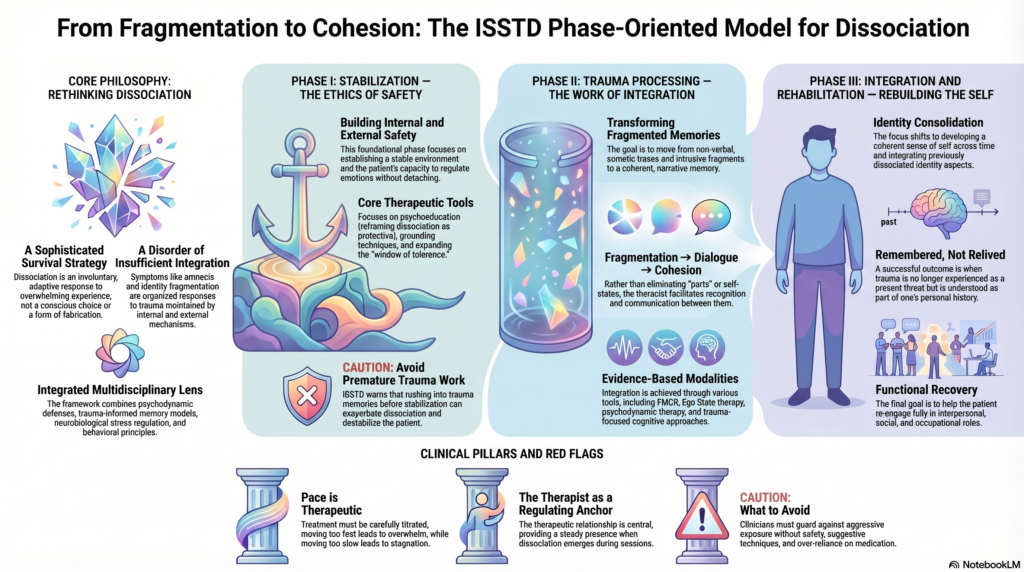
The significance of ISSTD lies not merely in its institutional authority, but in its integration of multiple paradigms:
- Psychodynamic understanding of defenses and fragmentation
- Trauma-informed models of memory and affect
- Neurobiological insights into stress and regulation
- Behavioral principles of reinforcement and avoidance
In doing so, ISSTD moves beyond reductionist explanations and offers a comprehensive, clinically usable framework.
🔷 The ISSTD Treatment Philosophy
At the heart of ISSTD’s guidelines is a fundamental shift in perspective:
Dissociation is not a disorder of excess—it is a disorder of insufficient integration.
Symptoms such as amnesia, depersonalization, identity fragmentation, or non-epileptic seizures are not random. They are organized responses to overwhelming experience, maintained by both internal and external mechanisms.
Therefore, treatment must not be abrupt or symptom-focused. It must be sequential, titrated, and integrative.
🟢 Phase I: Stabilization — The Ethics of Safety
ISSTD places extraordinary emphasis on the first phase of treatment. Contrary to common assumptions, this phase is not preparatory—it is foundational and often prolonged.
The primary task here is to establish:
- External safety (absence of ongoing trauma, stabilization of environment)
- Internal safety (capacity to regulate affect without dissociating)
Patients with dissociation often lack the ability to remain present under emotional stress. Their default response to overwhelming affect is detachment or fragmentation. Without addressing this, any attempt at trauma processing is not only ineffective but potentially harmful.
Thus, Phase I focuses on:
- Psychoeducation (reframing dissociation as protective)
- Grounding techniques (reconnecting to sensory reality)
- Affect regulation (expanding the window of tolerance)
- Behavioral stabilization (sleep, routine, substance control)
ISSTD explicitly cautions:
👉 Premature trauma work can exacerbate dissociation and destabilize the patient
This principle alone distinguishes expert care from poorly structured intervention.
🟡 Phase II: Trauma Processing — The Work of Integration
Only when sufficient stability is achieved does therapy progress to trauma processing.
Here, the task is not mere recollection, but transformation:
- From fragmented sensory-affective traces
- To coherent, narrative memory
Dissociated experiences are typically stored in:
- Non-verbal forms
- Somatic states
- Intrusive affective fragments
The clinician’s role is to facilitate their gradual integration, ensuring the patient remains within the window of tolerance.
ISSTD supports multiple modalities for this phase:
- Trauma-focused cognitive approaches
- EMDR (developed by Francine Shapiro)
- Psychodynamic therapy
- Parts-based (ego state) approaches
In complex dissociation, particularly DID, therapy often involves engaging with distinct self-states. ISSTD does not advocate confrontation or elimination of these states. Instead, it emphasizes:
- Recognition
- Communication
- Gradual integration
The movement is from:
👉 fragmentation → dialogue → cohesion
🔵 Phase III: Integration and Rehabilitation — Rebuilding the Self
In the final phase, the focus shifts from symptom reduction to identity consolidation and functional recovery.
The patient, having processed traumatic material, must now:
- Develop a coherent sense of self across time
- Integrate previously dissociated aspects of identity
- Re-engage with interpersonal and occupational roles
This phase is often overlooked but is crucial. Without it, patients may achieve symptom reduction without achieving psychological continuity.
A key transformation occurs here:
Trauma is no longer relived as present experience, but remembered as part of one’s history
🔷 Core Clinical Principles Emphasized by ISSTD
🔸 1. Dissociation is Involuntary and Adaptive
It is not malingering, not fabrication, and not under conscious control.
🔸 2. Treatment Must Be Phased
Skipping stabilization leads to:
- Symptom exacerbation
- Dropout
- Therapeutic rupture
🔸 3. Pace is Therapeutic
Too rapid → overwhelm
Too slow → stagnation
The art lies in titration
🔸 4. The Therapeutic Relationship is Central
Dissociation frequently emerges in-session:
- Sudden disengagement
- Affect shifts
- Identity changes
The therapist becomes a regulating anchor.
🔸 5. Parts Work is Valid
Self-states are not pathological entities to eliminate, but dissociated aspects of a unified personality to be integrated.
🔷 What ISSTD Cautions Against
- Aggressive trauma exposure without stabilization
- Suggestive techniques leading to false memory formation
- Over-reliance on pharmacotherapy
- Dismissing symptoms as “functional” in a pejorative sense
🔷 Clinical Relevance in Contemporary Practice
In modern psychiatric settings—especially in India—patients with dissociation often present across specialties:
- Psychiatry
- Neurology (PNES, unexplained seizures)
- General medicine
ISSTD’s framework provides:
- A shared language across disciplines
- A structured pathway for long-term care
- Protection against iatrogenic harm
📌 Final Synthesis
The contribution of ISSTD lies in transforming the treatment of dissociation from:
- Symptom suppression → process-oriented integration
- Fragmented approaches → coherent framework
- Reactive care → strategic, staged intervention
At its core, the ISSTD model recognizes a simple but profound truth:
Dissociation is not a failure of the mind—it is its most sophisticated survival strategy under unbearable conditions.
Treatment, therefore, is not about dismantling this strategy abruptly, but about making it unnecessary—by restoring the mind’s capacity to integrate, regulate, and remain present.
✍️ About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
At the Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall), dissociative disorders and trauma-related conditions are managed using ISSTD-aligned, phase-oriented treatment frameworks, integrated with:
- Psychodynamic formulation
- Objective assessment tools (QEEG, cognitive profiling where indicated)
- Evidence-based, individualized therapy
For individuals struggling with dissociation, trauma, or unexplained neurological symptoms, a structured and safe approach can transform outcomes.
✉ srinivasaiims@gmail.com 📞 +91-8595155808