Beyond Self-Report: Single-Visit ADHD Diagnosis Using Clinical Interview + QEEG + CPT in Chennai
 For decades, ADHD diagnosis has relied heavily on what patients say about themselves.
For decades, ADHD diagnosis has relied heavily on what patients say about themselves.
And that is precisely where the problem begins.
- Memory is imperfect
- Insight varies
- Symptoms overlap with anxiety, depression, personality traits
- And at times, symptoms may be unintentionally or intentionally exaggerated
In fact, modern research highlights that adult ADHD diagnosis is particularly vulnerable to subjective bias, making accurate identification challenging.
This is why psychiatry is now moving toward objective, multimodal diagnostic models.
The Shift: From Self-Report to Measurable Psychiatry
At institutions like the National University of Singapore, researchers have already demonstrated a new model of ADHD diagnosis that integrates:
- Clinical interview
- Questionnaires
- Objective tests (brain-based + behavioural)
Their approach combines:
- Brain function measurement
- Eye movement tracking
- Continuous performance testing
— all alongside traditional psychiatric evaluation.
Why?
Because no single method is enough.
Each modality captures a different layer:
- Subjective experience
- Behavioural performance
- Neurophysiological function
And when combined, diagnostic accuracy improves significantly.
What We Have Brought to Chennai
At Apollo Clinic Velachery, this multimodal, objective framework is now clinically implemented, adapted to real-world psychiatric practice.
Not as a replacement for clinical judgement —
but as a reinforcement of it.
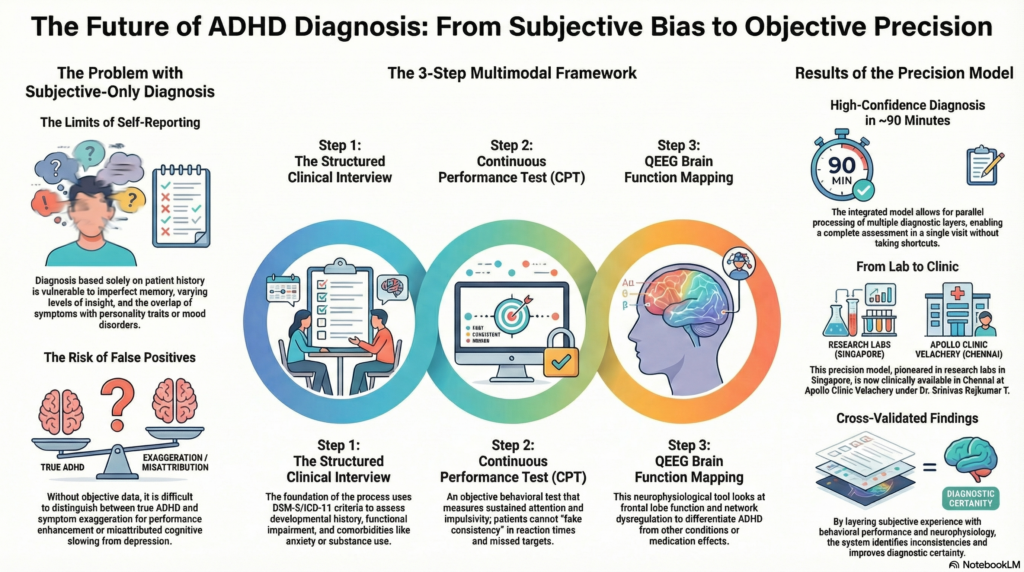
Step 1: Structured Clinical Interview (The Foundation)
A detailed, structured clinical interview
This includes:
- Developmental history (childhood onset)
- Functional impairment across settings
- Academic / occupational trajectory
- Comorbidities (anxiety, depression, substance use)
- Personality patterns
We also apply:
- DSM-5 / ICD-11 criteria
- Standardised rating scales
👉 This ensures that diagnosis is clinically valid and guideline-based
But here is the key shift:
We do not stop at self-report.
Step 2: Continuous Performance Test (CPT) – Measuring Attention Objectively
CPT evaluates:
- Sustained attention
- Impulsivity
- Reaction time variability
Patients cannot “fake consistency” here.
Typical ADHD patterns include:
- Increased commission errors
- Missed targets
- Fluctuating reaction times
These are quantifiable markers, not opinions.
Step 3: QEEG – Looking at Brain Function
QEEG provides:
- Objective mapping of brain activity
- Insights into frontal lobe function
- Network-level dysregulation
Research shows that neurophysiological tools like EEG and fNIRS can enhance diagnostic differentiation and monitoring, especially when combined with clinical assessment.
This helps answer critical questions:
- Is this ADHD or anxiety?
- Is this depression-related cognitive slowing?
- Is this medication effect?
Why This Matters: Eliminating False Positives
One of the concerns raised even in international research is:
👉 Overdiagnosis due to exaggerated self-reporting
There is documented concern that individuals may:
- Overestimate symptoms
- Seek diagnosis for performance enhancement
- Or misattribute other issues to ADHD
A purely interview-based system may struggle here.
But a multimodal system:
- Cross-validates findings
- Identifies inconsistencies
- Improves diagnostic confidence
Single Visit — Not Shortcut, But Integration
The NUS model demonstrates that a full ADHD assessment can be completed in ~90 minutes when structured properly.
Similarly, by integrating:
- Clinical interview
- CPT
- QEEG
👉 We are able to arrive at a high-confidence diagnosis within a single visit
This is not:
- Rushed
- Superficial
- Or shortcut-based
This is:
Parallel processing of multiple diagnostic layers
From Diagnosis to Treatment (Same Day, When Indicated)
Once diagnosis is established:
- A structured formulation is made
- Comorbidities are addressed
- Treatment is initiated
Including medications like Methylphenidate
— prescribed strictly as per regulatory guidelines
Precision Psychiatry — Now a Reality
What was once confined to research labs in Singapore is now:
👉 Clinically available in Chennai
A model where:
- Psychiatry is not just descriptive
- But increasingly measurable, objective, and precise
Who Should Consider This?
- Adults unsure about ADHD diagnosis
- Patients with partial / unclear previous assessments
- Individuals with overlapping anxiety or depression
- Students and professionals needing clarity before treatment
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
With a clinical approach that integrates structured interviews, neurotechnology, and objective cognitive testing, Dr. Srinivas focuses on accurate diagnosis, reduced uncertainty, and evidence-based care in ADHD and related conditions.