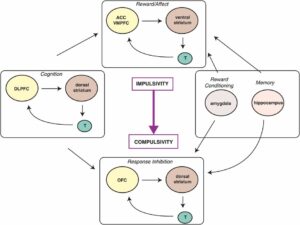
ACC (Anterior Cingulate Cortex) and VMPFC (Ventromedial Prefrontal Cortex):
These regions govern decision-making, emotional regulation, and impulse control.
Dysfunction in these areas leads to impaired inhibition, resulting in impulsive actions.
Ventral Striatum:
Central to reward processing and the drive for immediate gratification.
Dopaminergic activity in this region plays a critical role in impulsive decision-making.
Thalamus:
Acts as a relay station, linking cortical regions with striatal systems to process sensory inputs and facilitate action.
Disorders Associated with Impulsivity:
Includes ADHD, mania, borderline personality disorder, antisocial behaviors, and impulse control disorders like kleptomania and pyromania.
Characterized by difficulty delaying gratification and susceptibility to immediate rewards or actions.
Compulsivity: Neural and Behavioral Aspects
Key Brain Areas:
OFC (Orbitofrontal Cortex):
Associated with decision-making, valuation of actions, and habit formation.
Dysfunction here results in rigid, repetitive, and goal-insensitive behaviors.
Dorsal Striatum:
Dominates in the compulsivity phase, reinforcing habitual actions irrespective of outcomes.
Plays a significant role in the progression to compulsive behaviors through habit circuit adaptations.
Thalamus:
Facilitates communication between cortical and striatal regions, ensuring habitual responses are executed efficiently.
Disorders Associated with Compulsivity:
Includes OCD, Tourette syndrome, trichotillomania, hypochondriasis, and compulsive shopping or gambling.
Defined by repetitive, rigid behaviors aimed at reducing anxiety or achieving a sense of control.
Transition from Impulsivity to Compulsivity
The transition involves:
Neuroplastic Changes: Shifts in synaptic strength from ventral (reward-driven) to dorsal (habit-driven) circuits.
Behavioral Adaptation: Movement from seeking immediate gratification to engaging in repetitive, rigid actions, even at the expense of negative consequences.
Mechanisms:
Over time, dopaminergic dysregulation shifts from phasic (ventral striatum) to tonic activity (dorsal striatum), strengthening habits.
Glutamatergic and GABAergic imbalances disrupt cortical inhibition, making it harder to override compulsive behaviors.
Clinical Implications and Treatments
For Impulsivity:
Targeting prefrontal control mechanisms with therapies like cognitive-behavioral therapy (CBT) or medications that enhance dopamine and serotonin signaling.
Disorders like ADHD may benefit from stimulant medications that modulate dopaminergic pathways.
For Compulsivity:
Treatments aimed at disrupting habitual circuits (e.g., selective serotonin reuptake inhibitors for OCD) or deep brain stimulation targeting the striatal regions.
Psychosocial interventions to improve cognitive flexibility and adaptive behaviors.
Integration with Psychiatric Disorders
This model illustrates the overlap of impulsivity and compulsivity with a variety of disorders. For example:
Drug addiction spans both domains, beginning with impulsive use for reward and progressing to compulsive seeking despite harm.
Gambling disorder often evolves similarly, driven first by thrill-seeking (impulsivity) and later by repetitive, compulsive behaviors.